Real-world ALS progression data after MSEC treatment
Amyotrophic lateral sclerosis, commonly known as ALS, is a progressive neurodegenerative disease that affects motor neurons. These are the nerve cells responsible for voluntary movement, including walking, speaking, swallowing and breathing. As ALS progresses, patients can lose function at very different speeds. Some people decline rapidly, while others remain relatively stable for longer periods.
This variability is one of the central challenges in ALS research. When a patient remains stable after treatment, it is difficult to know whether the treatment influenced the disease course or whether the patient was already a naturally slow progressor. Likewise, when a patient declines quickly, this may reflect aggressive disease biology rather than treatment failure.
For this reason, structured follow-up data is important. At ANOVA, we reviewed real-world ALSFRS-R progression data from patients who received MSEC treatment. The goal of this analysis was not to prove efficacy, but to better understand whether the observed functional decline in treated patients differed from expected progression rates reported in the scientific literature.
The results showed a numerically slower average decline than selected literature reference slopes. However, the differences were not statistically significant. This means the findings should be interpreted as an exploratory clinical signal, not as proof that MSEC slows ALS progression.
What is MSEC?
MSEC stands for mesenchymal stem cell secretome. Unlike direct stem cell transplantation, secretome-based approaches focus on the biologically active factors released by mesenchymal stem cells, including extracellular vesicles, proteins, cytokines and other signaling molecules.
In regenerative medicine, the secretome is studied because many effects of mesenchymal stem cells may be mediated not by permanent engraftment of cells, but by the signals these cells release. These signals are being investigated for their potential roles in inflammation, tissue repair, immune modulation and cell-to-cell communication.
In ALS, this biological rationale is experimental. ALS is a complex neurodegenerative disease, and no secretome-based therapy should be presented as a cure or as a proven disease-modifying treatment. The purpose of this article is therefore to present real-world observational data transparently and to explain what it may and may not suggest.
Why ALSFRS-R is used to measure ALS progression
The ALS Functional Rating Scale-Revised, or ALSFRS-R, is one of the most widely used tools to monitor functional status in ALS. It evaluates daily functions such as speech, swallowing, handwriting, walking, breathing and other motor activities.
The maximum ALSFRS-R score is 48 points. A higher score indicates better function. A lower score indicates greater functional impairment. In ALS research, one isolated score is less informative than the rate of change over time. For example, a patient whose ALSFRS-R score decreases by one point per month is progressing differently from a patient whose score decreases by only 0.3 points per month.
For this reason, our analysis focused on the ALSFRS-R slope, meaning the average number of points lost per month.
How the ANOVA real-world cohort was analyzed
We reviewed ALSFRS-R follow-up data from patients who received MSEC treatment at ANOVA. Month 0 was defined as the reference point around the time of liposuction/cell preparation. Follow-up scores were then tracked over time.
The analysis included:
- Individual ALSFRS-R trajectories after MSEC treatment
- Mean ALSFRS-R development over 24 months
- Comparison with literature reference slopes for untreated ALS and riluzole-treated ALS
- Linear regression slope analysis per patient
- Subgroup analysis of slow, intermediate and fast progressors
The full follow-up analysis included 69 patients. A separate first-9-month analysis included 66 patients. Some patients had long follow-up, while others had only two or a few data points. This is important because short follow-up can make slope estimates less reliable.
This was a real-world observational analysis. It was not a randomized controlled trial. There was no matched placebo group. Therefore, the findings must be interpreted cautiously.
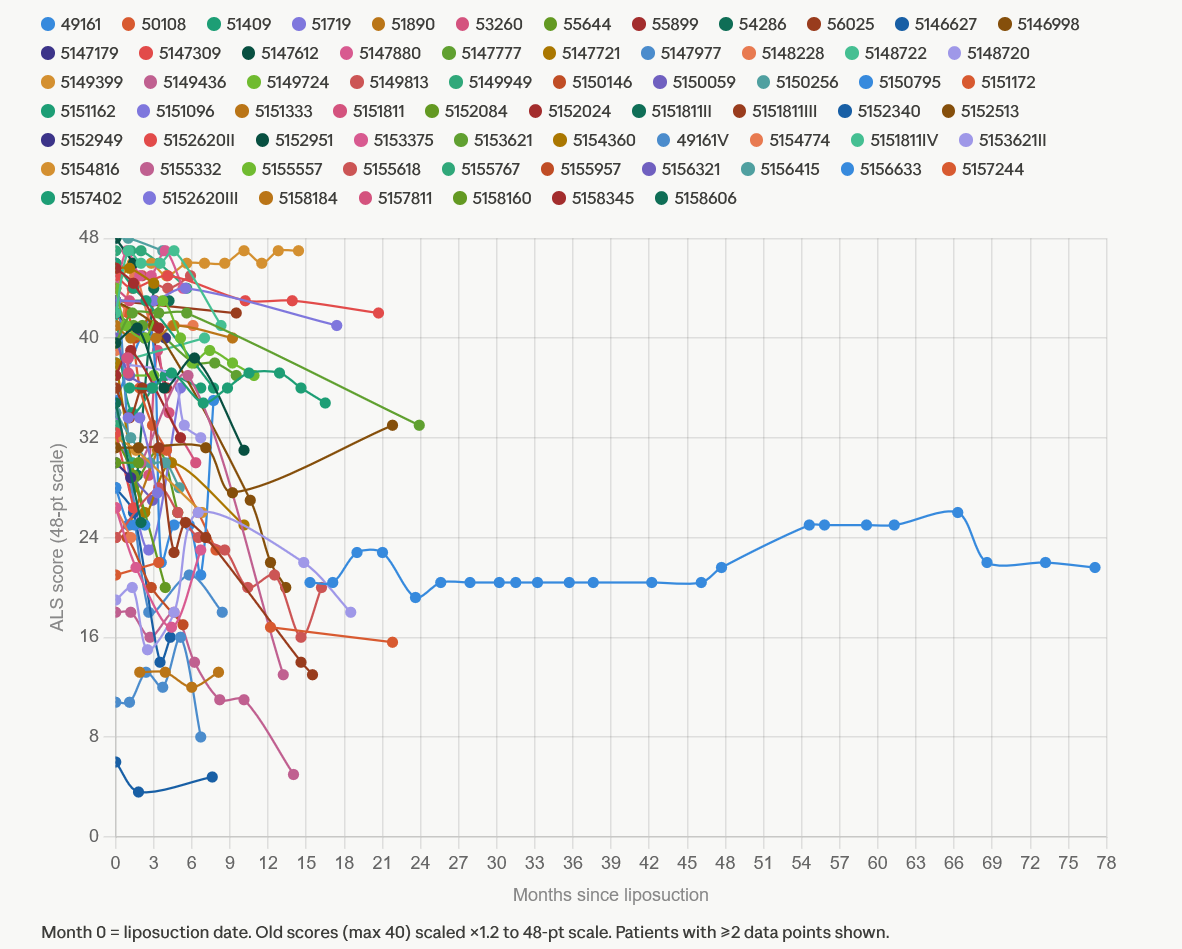
Individual ALSFRS-R trajectories show high variability
The individual patient trajectories show one of the most important realities of ALS: progression is highly variable.
Some patients in the cohort showed steep decline. Others showed relatively stable ALSFRS-R scores for several months. A few patients had longer follow-up periods and appeared to remain within a relatively narrow functional range over time.
This type of graph is useful because it prevents oversimplification. Looking only at a mean curve can hide the fact that ALS does not progress in the same way in every patient. Individual lines show the real-world heterogeneity of the disease.
For patients and families, this is important. A single patient story, whether positive or negative, cannot reliably prove whether a therapy is working. ALS progression must be interpreted across a larger group and over time.
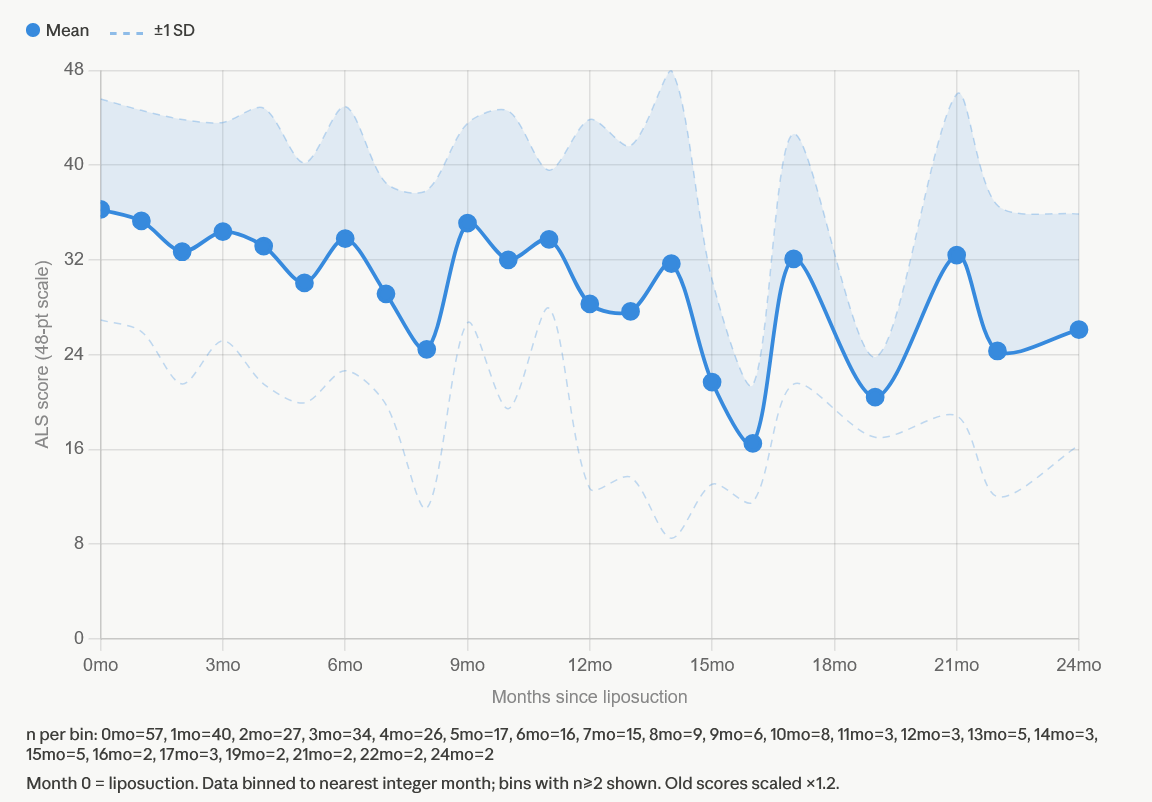
Mean ALSFRS-R development after MSEC treatment
When the patient data was grouped by month, the mean ALSFRS-R curve showed a slower average decline than might be expected in a typical ALS population. However, the graph also shows substantial variability, represented by the wide shaded area.
This variability matters. In ALS, standard deviation can be large because patients differ strongly in disease stage, baseline score, progression speed, respiratory status, bulbar involvement, age, genetics and follow-up duration.
The number of patients contributing to each monthly time point also changes over time. Early months include more patients. Later months include fewer patients, which makes the mean more sensitive to individual outliers. For that reason, the later part of the curve should not be overinterpreted.
The mean curve is therefore useful as a descriptive overview, but it does not by itself prove a treatment effect.
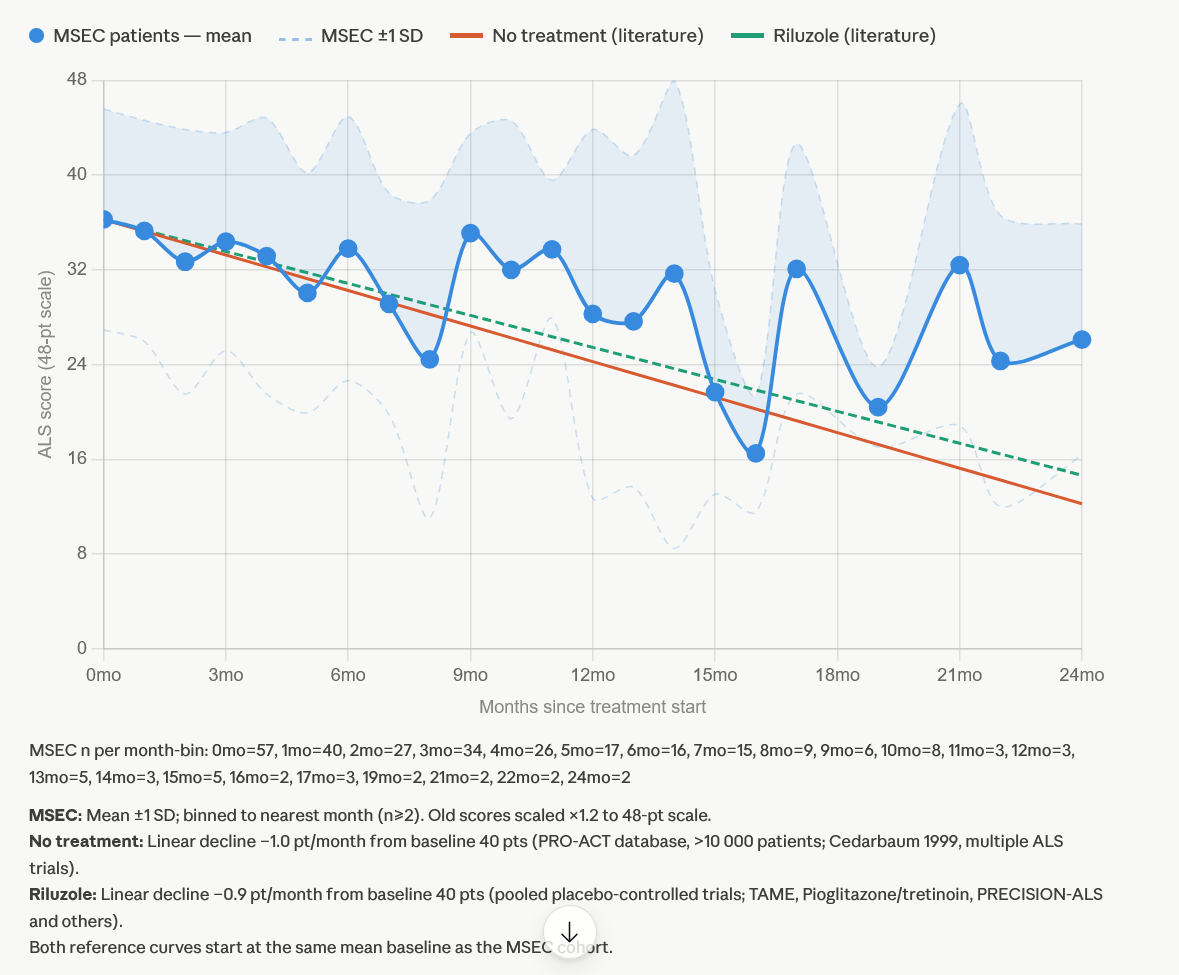
Comparison with literature reference slopes
To provide context, the MSEC cohort was compared with two literature-derived reference slopes:
- An untreated ALS reference slope of approximately –1.0 ALSFRS-R point per month
- A riluzole-treated reference slope of approximately –0.9 ALSFRS-R points per month
In the MSEC cohort, the observed average decline was:
- –0.697 points per month over full follow-up
- –0.632 points per month during the first 9 months
Numerically, this suggests that the MSEC cohort declined more slowly than the selected reference slopes.
Compared with the untreated reference slope of –1.0 point per month, the full follow-up MSEC slope of –0.697 points per month was approximately 30% slower. During the first 9 months, the MSEC slope of –0.632 points per month was approximately 37% slower.
Compared with the riluzole reference slope of –0.9 points per month, the full follow-up MSEC slope was approximately 23% slower. During the first 9 months, it was approximately 30% slower.
These numbers are clinically interesting. However, they must be interpreted correctly. A numerical difference does not automatically mean that the treatment caused the difference. Statistical testing is needed to estimate whether the observed difference is likely to reflect a true effect rather than random variation or patient selection.
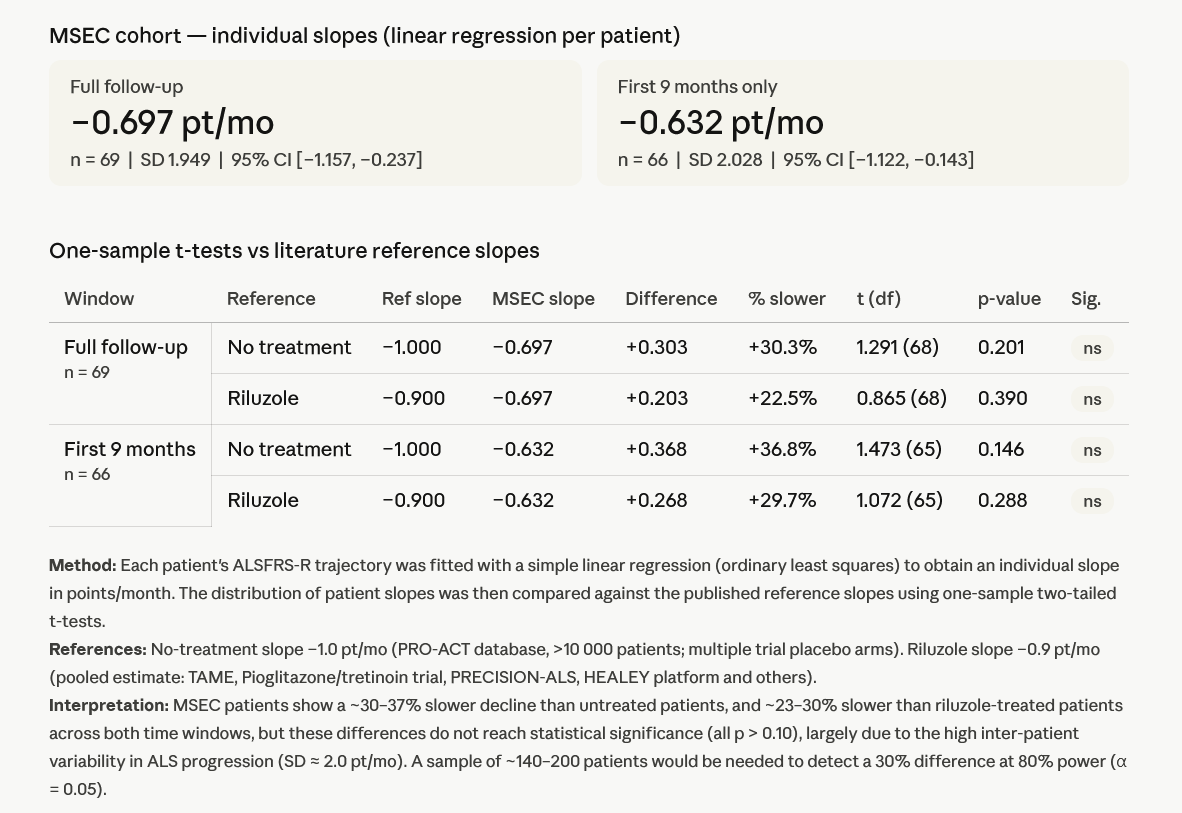
Statistical interpretation: slower numerical decline, but not statistically significant
The slope analysis showed the following:
| Analysis window | MSEC slope | Reference | Reference slope | Difference | Approximate numerical reduction |
|---|---|---|---|---|---|
| Full follow-up | –0.697 pt/month | No treatment | –1.0 pt/month | +0.303 pt/month | 30.3% slower |
| Full follow-up | –0.697 pt/month | Riluzole | –0.9 pt/month | +0.203 pt/month | 22.5% slower |
| First 9 months | –0.632 pt/month | No treatment | –1.0 pt/month | +0.368 pt/month | 36.8% slower |
| First 9 months | –0.632 pt/month | Riluzole | –0.9 pt/month | +0.268 pt/month | 29.7% slower |
However, the p-values were not statistically significant:
| Comparison | p-value | Interpretation |
|---|---|---|
| Full follow-up vs untreated reference | 0.201 | Not statistically significant |
| Full follow-up vs riluzole reference | 0.390 | Not statistically significant |
| First 9 months vs untreated reference | 0.146 | Not statistically significant |
| First 9 months vs riluzole reference | 0.288 | Not statistically significant |
This means that although the MSEC cohort declined more slowly on average, the analysis cannot prove that MSEC caused the slower decline.
The reason is not necessarily that the observed difference is meaningless. Rather, ALS progression is highly variable, and the cohort size was limited. The analysis estimated that approximately 140–200 patients would be needed to detect a 30% difference with 80% statistical power at alpha = 0.05.
In other words, the data shows a clinically interesting signal, but the current sample is underpowered for definitive conclusions.
What this data may suggest
The real-world data may suggest that ALS patients treated with MSEC had a slower average ALSFRS-R decline than selected literature reference slopes. The magnitude of the numerical difference, approximately 30–37% compared with untreated reference progression, is large enough to be clinically interesting.
The data also supports an important practical observation: ALS patients are not one uniform group. Some patients remain stable for longer periods, while others decline very quickly. Any future study of MSEC in ALS would need to account for baseline progression speed, disease duration, respiratory status, bulbar involvement, genetic subtype, standard medication use and follow-up duration.
The most responsible interpretation is that this real-world analysis provides a signal worth further structured investigation.
What this data does not prove
This analysis does not prove that MSEC slows ALS progression.
It also does not prove that MSEC is superior to riluzole, edaravone, tofersen or any other approved or standard ALS therapy. Patients should not discontinue prescribed ALS medications or supportive care because of this analysis.
The data also cannot exclude selection bias. Patients who receive and return for regenerative medicine treatments may differ from the broader ALS population in important ways. They may have different disease stages, different access to care, different baseline progression rates, different motivation to pursue follow-up or different survival characteristics.
The data also cannot determine how much of the observed effect may be related to MSEC, standard medication, supportive care, natural slow progression or other factors.
For these reasons, this analysis should be understood as real-world observational data, not as proof of efficacy.
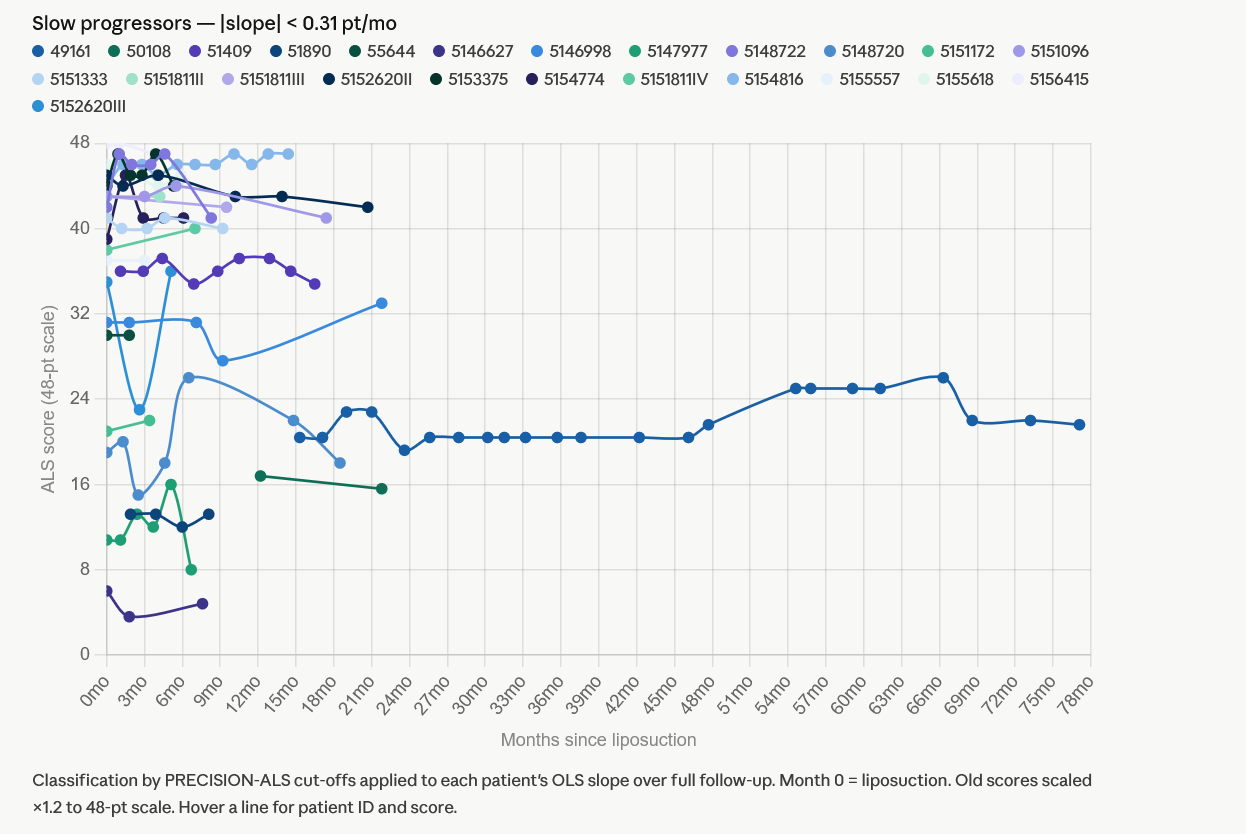
Slow, intermediate and fast ALS progressors
To better understand the variability in the cohort, patients were classified into three progression groups using published PRECISION-ALS cut-offs:
- Slow progressors
- Intermediate progressors
- Fast progressors
The cohort split almost evenly across the three groups.
The slow progressor group included 24 patients. These patients had slopes below 0.31 ALSFRS-R points per month. Some showed near-flat or slightly improving trajectories. However, slow progression can occur naturally in ALS and should not be assumed to result from treatment.
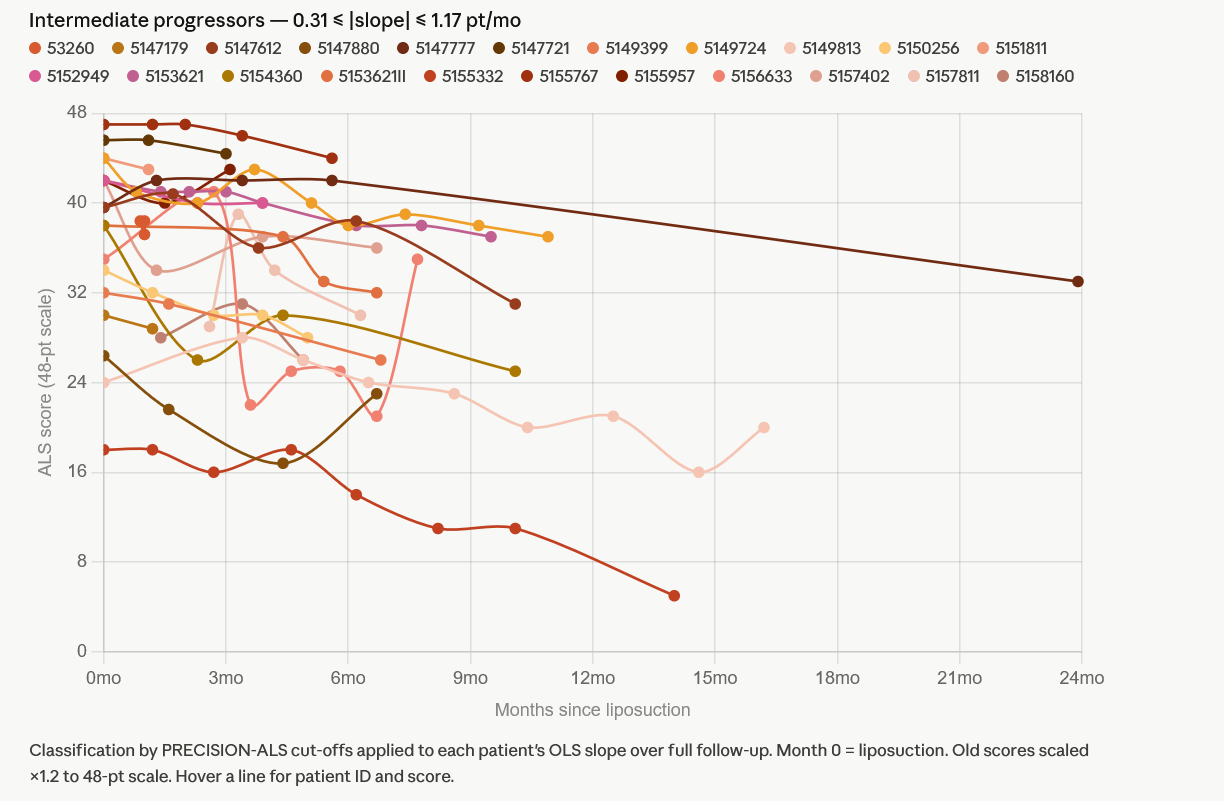
The intermediate progressor group included 22 patients. These patients declined at a rate between 0.31 and 1.17 ALSFRS-R points per month. This group is especially important because it may resemble the typical progression range seen in many ALS cohorts.
For future analysis, this group may be more informative than the full mixed cohort because it excludes both very slow and very fast outliers.
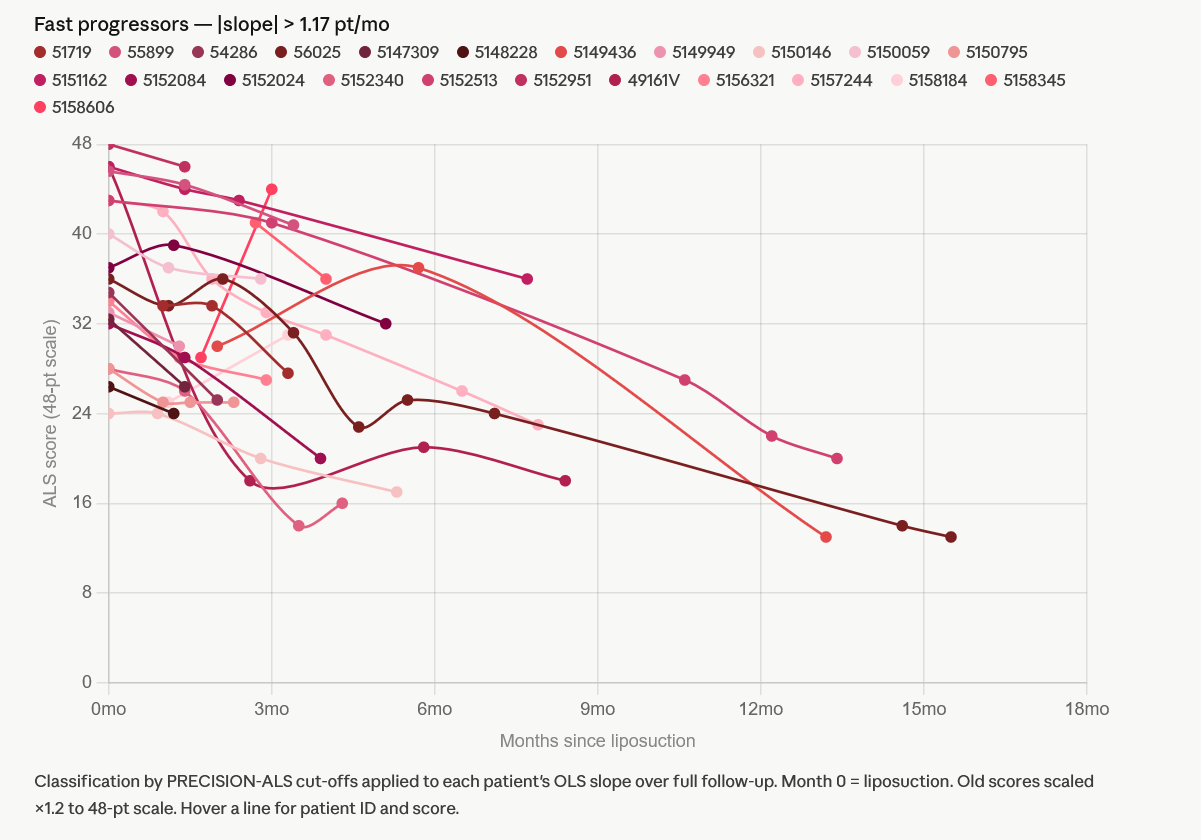
The fast progressor group included 23 patients. These patients had slopes above 1.17 ALSFRS-R points per month. This group showed the steepest functional decline.
Some patients in this category had very short follow-up, sometimes with only two data points. Short follow-up can make the calculated slope appear especially steep. Therefore, these results should be interpreted with caution.
This subgroup highlights why ALS real-world data must be analyzed carefully. If fast progressors and slow progressors are combined without adjustment, the average can become difficult to interpret.
Main limitations of this real-world ALS analysis
Several limitations must be clearly acknowledged.
First, this was not a randomized controlled trial. Without a matched control group, it is impossible to determine whether the observed slower decline was caused by MSEC.
Second, the comparison used literature reference slopes. Literature references are useful for context, but they are not equivalent to a control group treated at the same time, under the same conditions, with the same inclusion criteria.
Third, patient characteristics varied. ALS patients may differ in disease duration, baseline ALSFRS-R score, progression speed, respiratory function, bulbar symptoms, genetic background, standard medication use and supportive care.
Fourth, some patients had short follow-up. When a patient has only two or a few data points, the slope estimate may be less reliable.
Fifth, survival bias may play a role. Patients who return for additional visits and follow-up may be patients who are doing better, while patients with rapid deterioration may be less likely to continue follow-up.
These limitations do not make the data useless. They simply define what the data can and cannot tell us.
Why this data is still worth presenting
Despite the limitations, real-world data can be valuable when presented transparently.
ALS is a severe disease with limited treatment options. Patients and physicians need honest information about experimental approaches, including both potential signals and uncertainty. Publishing only success stories can be misleading. Publishing structured cohort data, including limitations and non-significant results, provides a more responsible basis for discussion.
The MSEC cohort showed a numerically slower average ALSFRS-R decline than selected reference slopes. The result was not statistically significant, but the direction and magnitude of the signal justify further analysis and, ideally, more structured prospective research.
For ANOVA, this type of transparent data presentation is important. It allows patients to understand that MSEC is not being presented as a guaranteed ALS therapy, but as an experimental regenerative medicine approach being evaluated through real-world follow-up.
How patients should interpret this information
Patients with ALS should interpret this article carefully.
The data does not mean that MSEC will slow progression in an individual patient. It does not mean that a patient can expect stabilization or improvement. It does not replace standard neurological care, respiratory support, nutritional care, physiotherapy, speech therapy or approved ALS medications.
Instead, the data may help patients ask better questions:
- What is my current ALSFRS-R score?
- How fast has my ALSFRS-R score changed over the past months?
- Am I a slow, intermediate or fast progressor?
- Which standard ALS treatments am I currently receiving?
- What are realistic goals for experimental treatment?
- How will treatment response be monitored?
- What follow-up data will be collected?
These questions are essential because ALS treatment decisions should be individualized and medically supervised.
MSEC treatment at ANOVA: an experimental context
At ANOVA, MSEC is part of a regenerative medicine approach using autologous mesenchymal stem cell-derived secretome. The treatment concept is based on the biological activity of stem cell-derived signaling factors rather than direct replacement of motor neurons.
In ALS, this approach remains experimental. It should not be described as curative, proven or guaranteed to stop disease progression. The current real-world analysis provides observational data that may support further investigation, but it does not establish clinical efficacy.
Patients interested in MSEC should undergo individual medical review. This includes diagnosis confirmation, disease history, current medications, ALSFRS-R history, respiratory status, swallowing status, imaging and relevant laboratory findings.
Conclusion: an encouraging signal, not proof
In this real-world cohort of ALS patients treated with MSEC, the average ALSFRS-R decline was numerically slower than selected literature reference slopes.
The full follow-up analysis showed an average decline of approximately –0.697 ALSFRS-R points per month. During the first 9 months, the average decline was approximately –0.632 points per month. These values were slower than the reference slopes used for untreated ALS and riluzole-treated ALS.
However, the differences were not statistically significant. The analysis was observational, non-randomized and underpowered. It therefore cannot prove that MSEC slows ALS progression.
The most responsible conclusion is that the ANOVA real-world data shows an interesting clinical signal that warrants further structured investigation. For patients, it may provide useful context, but it should not be interpreted as a guarantee of benefit.
Request an individual ALS case review
Patients and families interested in MSEC for ALS can get in touch for an individual case review. Useful documents include neurological reports, ALSFRS-R history, medication list, respiratory function tests, genetic testing if available, imaging, and a summary of disease onset and progression.
ANOVA reviews each case individually to assess whether regenerative medicine treatment may be medically appropriate and whether realistic treatment goals can be defined.