
Amyotrophic Lateral Sclerosis (ALS) Treatment Options
Amyotrophic Lateral Sclerosis (ALS) Treatment Options
Amyotrophic lateral sclerosis (ALS), also known as Lou Gehrig’s disease, is a progressive motor neuron disease. ALS affects the nerve cells that help control voluntary muscle movement. As the disease progresses, patients may experience symptoms such as:
- Muscle twitching or cramps
- Worsening muscle weakness
- Mobility loss
- Speech changes
- Swallowing difficulty
- Breathing problems
There is currently no cure for ALS. Instead, standard treatment focuses on slowing progression where possible, managing symptoms and supporting quality of life through a multidisciplinary treatment plan.
ALS Treatment Options: Quick Comparison
|
Treatment option |
Care area |
Main goal |
Key consideration |
|---|---|---|---|
|
ALS medication |
Modestly slow ALS progression and support survival |
Requires physician monitoring and does not reverse motor neuron damage |
|
|
Gene-targeted ALS medication |
Treat SOD1-associated ALS |
Only relevant for adults with confirmed SOD1-ALS |
|
|
ALS medication approved in some countries |
May slow functional decline in selected patients |
Approved in some countries, including the U.S., but not currently authorized by the EMA as an ALS treatment in the EU |
|
|
Symptom-focused medication |
Improve comfort and quality of life |
Help manage symptoms but do not stop ALS progression |
|
|
Supportive therapy |
Support mobility, posture, comfort, and safe activity |
Should be adjusted to disease stage, weakness, and fatigue level |
|
|
Supportive therapy |
Help maintain independence with daily activities |
May include adaptive equipment, assistive devices, and home safety support |
|
|
Supportive therapy |
Support speech, swallowing assessment, and communication planning |
Early planning can help preserve communication options |
|
|
Supportive care |
Support weight, hydration, and safer swallowing |
May include diet changes, supplements, or feeding tube discussion |
|
|
Respiratory support |
Assist breathing and airway clearance |
May include noninvasive ventilation, secretion support, or tracheostomy discussion |
|
|
Whole-person support |
Support emotional health, care planning, and quality of life |
Palliative care can be provided alongside active ALS care |
|
|
Clinical trials |
Study possible new ALS medications |
Eligibility varies by study, and benefit is not guaranteed |
|
|
Clinical trials / precision medicine |
Explore treatment approaches based on genetics, biomarkers, or ALS subtype |
Some approaches are only relevant for specific genetic forms of ALS |
|
|
Experimental regenerative research |
Explore possible effects on neuroprotection, inflammatory signalling, cellular stress, and the nerve-cell environment |
Experimental; not a cure or replacement for standard ALS care |
Medications Used in ALS Treatment
Medications, like other ALS treatments, do not cure ALS or reverse motor neuron damage. Instead, modern treatment plans may combine medications that slow disease progression with drugs that relieve specific symptoms.
The exact plan depends on physician review, including the patient’s diagnosis, disease stage, genetic subtype, symptoms, overall health and local medication availability.
Medication availability can change over time. For example, Relyvrio/Albrioza was voluntarily discontinued in the U.S. and Canada in 2024 after the Phase 3 PHOENIX trial did not confirm benefit. Patients should ask their neurologist which medications are currently available and appropriate in their country.
Riluzole (Rilutek®, Exservan® and Tiglutik®)
After receiving FDA approval in 1995 and EU marketing authorization in 1996, riluzole became one of the main medications used in ALS treatment. It is available in different oral forms, including tablets, oral film, and oral suspension, depending on the specific product and country.
Riluzole has shown the potential to modestly slow ALS disease progression and may help extend life or the time to mechanical ventilation.
Common side effects may include:
- Dizziness
- Gastrointestinal side effects
- Liver problems
As a result, patients typically require physician monitoring while taking the medication.
Tofersen (Qalsody®)
Sold under the brand name Qalsody®, tofersen was granted accelerated FDA approval in 2023 and EU marketing authorization under exceptional circumstances in 2024 to treat ALS associated with SOD1 mutations. As a result, it is not relevant for most ALS patients, and confirmation of an SOD1 mutation is needed to determine eligibility.
Tofersen should be discussed with a neurologist familiar with genetic ALS treatment.
Edaravone (Approved in Some Countries, Not Authorized in the EU)
Edaravone is an antioxidant treatment that received FDA approval for ALS in 2017. However, it is not currently authorized as a standard ALS treatment in the EU.
Edaravone can be delivered through a vein in the arm or taken orally, depending on the specific product and country. It is intended to reduce oxidative stress, a process being studied in ALS-related motor neuron damage. In selected ALS patients, it may help slow functional decline.
Potential benefits for lifespan are currently less clear, while possible side effects include:
- Bruising
- Headache
- Problems walking
Suitability depends on physician review, disease stage, overall health, local medication availability, and treatment goals.
Symptom Management Medications
Alongside medications intended to slow ALS progression, physicians may also recommend symptom-focused medications to manage complications and improve comfort.
These medications may help with ALS-related symptoms such as:
- Muscle cramps
- Spasticity
- Pain
- Excess saliva
- Sleep problems
- Constipation
- Depression or anxiety
- Pseudobulbar affect
While symptom management medications can help improve quality of life, they do not stop ALS progression or reverse established motor neuron damage.

ALS Supportive Therapies and Multidisciplinary Care
Treatment often involves more than medication alone. Supportive therapies do not cure ALS or modify the disease itself, but they can help people with ALS preserve daily function, independence, and quality of life.
The sections below explain how different supportive therapies may help ALS patients adapt as their symptoms change.
Physical Therapy
Physical therapy can help ALS patients adapt to their symptoms and preserve function for as long as possible.
Some potential benefits of physical therapy include:
- Maintaining mobility, flexibility, posture, comfort, and remaining muscle strength
- Helping manage pain and discomfort
- Supporting cardiovascular fitness in appropriate patients
Because ALS-related weakness and fatigue can worsen function, physical therapy should always be adapted to the patient’s disease stage and fatigue level, with activity plans developed in coordination with a physical therapist.
Occupational Therapy
Occupational therapy can help ALS patients maintain independence with daily activities as hand, arm, and mobility function changes.
An occupational therapist may recommend practical supports such as adaptive equipment, assistive technology and home safety adjustments to make daily routines safer and reduce caregiver strain.
Speech Therapy and Communication Support
Speech therapy can help ALS patients maintain communication as speech, voice, and swallowing symptoms progress.
A speech-language pathologist can help with speech clarity, swallowing assessment and communication planning. In many cases, this may include voice banking or technology such as speech-generating devices, text-to-speech tools and eye-tracking systems.
Early planning can help patients preserve communication options before speech becomes severely affected.
Nutritional Support
As symptoms progress, swallowing difficulties can make it harder to eat, contributing to weight loss in ALS patients. Proper nutritional support from a dietitian can help patients maintain weight, which may be associated with better outcomes.
Nutritional support from a dietitian may include:
- Higher-calorie meals
- Texture-modified foods
- Thickened liquids
- Meal timing adjustments
- Supplements, when appropriate
When swallowing becomes too difficult, nutritional support may also include the use of feeding tubes. These can help reduce risks associated with difficult swallowing while supporting hydration, nutrition, and medication intake.
The decision to use a feeding tube should be made collaboratively with the patient, family, neurologist, dietitian, and speech-language pathologist.
Breathing Support
ALS can weaken the muscles involved in breathing, making respiratory support important as symptoms progress.
Respiratory support may include:
- Noninvasive ventilation, such as BiPAP
- Assisted coughing devices
- Suction devices to help clear secretions
- Tracheostomy ventilation in selected advanced cases
In some cases, tracheostomy ventilation may be considered when noninvasive ventilation is no longer enough or when patients choose long-term invasive ventilation.
A tracheostomy is a major decision involving quality of life, planning and caregiver support. Patients and families should discuss breathing support early with their ALS clinical team to understand the medical, practical, emotional and home-care implications.
Psychological, Social, and Palliative Support
ALS can place emotional, financial and caregiving strain on patients and families. Psychological and social support may include counselling, social work, caregiver support and advance care planning.
Palliative care does not mean stopping ALS treatment. Instead, it can help with symptom management, decision-making, emotional support and quality of life.
Social support can also help patients access equipment, home care, benefits, transportation and community resources.

Experimental Therapies and ALS Clinical Trials
Beyond current medications and supportive therapies, ALS research continues to evolve as scientists learn more about motor neuron degeneration, genetic subtypes of ALS, disease biomarkers, and the biological environment surrounding affected nerve cells.
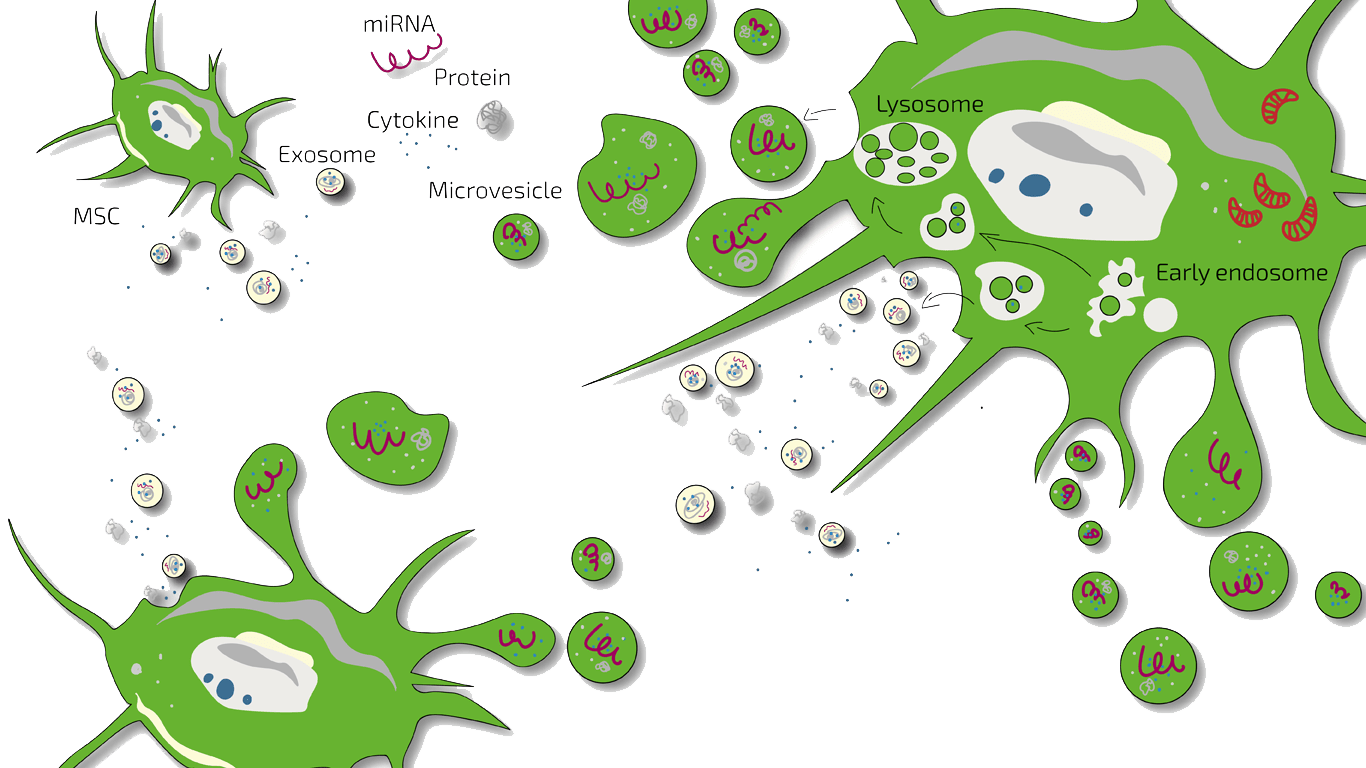
Emerging areas of ALS research include investigational drugs, gene-targeted approaches, biomarker research, precision medicine, cell-based therapies,stem cell secretome and extracellular vesicle research, and regenerative medicine research.
Investigational therapies are usually studied through clinical trials before they become part of standard ALS care. Eligibility varies by study, and benefit is not guaranteed.
Experimental ALS therapies are not cures and should never replace standard neurological care, respiratory support, nutritional support, or multidisciplinary ALS management.
Investigational Drug Trials
Investigational drug trials study potential ALS medications that are not yet established as standard care. These trials may evaluate whether a therapy can slow functional decline, affect disease biomarkers, improve survival-related outcomes, or support better symptom control.
Some examples of ALS drug trials include:
- HEALEY ALS Platform Trial: Began in 2020 and has studied multiple investigational ALS treatments through a shared platform trial design. More than 1,300 people have participated in the platform trial.
- PREVAiLS Phase 3 trial: Began enrolling participants in 2026 to study pridopidine, an investigational drug being evaluated for ALS progression.
Participation in an ALS clinical trial depends on study criteria, disease stage, diagnosis, location, prior treatments, breathing function, and overall health. Eligibility varies, and benefit is not guaranteed.
Gene-Targeted and Precision Medicine Research
ALS research is also moving toward more individualized treatment approaches based on genetics, biomarkers, and disease subtype.
Gene-targeted and precision medicine research may focus on:
- Specific ALS-related mutations
- Biological pathways involved in disease progression
- Measurable disease markers
- Treatment approaches for defined patient subgroups
Tofersen is one example of howgenetic testing can affect ALS treatment decisions, since it is only relevant for patients with confirmed SOD1-associated ALS. Other gene-targeted and precision medicine approaches remain under investigation.
These approaches are still highly individualized and should be reviewed with a neurologist or ALS specialist.
Stem Cell and Regenerative Medicine Research
Stem cell-based therapy is another emerging area being explored for ALS. The current rationale is not based on replacing lost motor neurons or curing the disease. Instead, research has focused on whether these approaches may influence the biological environment around affected nerve cells.
Rather than claiming to rebuild damaged motor neurons, researchers are exploring possible effects on:
- Neuroprotection
- Inflammatory signalling
- Cellular stress
- Paracrine signalling
- Extracellular vesicle and secretome activity
At ANOVA-IRM,experimental regenerative medicine for ALS is reviewed through individualized medical assessment and case-by-case discussion. This may include stem cell secretome or extracellular vesicle/exosome-related approaches when medically appropriate.
Clinical use of stem cell-based therapy for ALS remains experimental. Suitability depends on diagnosis, disease stage, breathing and swallowing function, overall health, travel suitability, treatment goals, and benefit-risk assessment. Stem cell-based therapy cannot guarantee ALS improvement, disease stabilization, motor recovery, or survival extension.
Stem Cell Therapy Contraindications
Experimental regenerative therapy is not suitable for every ALS patient. ANOVA-IRM does not treat patients when certain risk factors are present, including:
- Active cancer within the last two years
- Being under the legal age for treatment
- Pregnancy or breastfeeding
- Ventilator dependence or inability to breathe independently
- Difficulty breathing while lying down
- Severe swallowing difficulty
- Severe or uncontrolled psychiatric conditions
- Active infectious disease, including hepatitis, HIV, syphilis, or other infections
Request an Individual Medical Review for ALS
If you or a family member has ALS, you can contact ANOVA-IRM to ask whether an individual medical review may be appropriate.
Before any experimental option is considered, ANOVA reviews each case individually. This may include diagnosis, disease stage, progression rate, breathing and swallowing function, current medications, overall health, travel suitability, and treatment goals.
Regenerative therapy cannot replace standard ALS care. Patients should continue working with their neurologist or ALS care team while exploring additional options.
FAQs About ALS Treatment Options
What are the treatment options for amyotrophic lateral sclerosis?
Treatment options for amyotrophic lateral sclerosis include ALS-specific medications, symptom management medications, supportive therapies, nutritional and breathing support, psychological and social support, palliative care, clinical trials, and experimental approaches such as stem cell treatment.
The right treatment plan depends on the patient’s diagnosis, disease stage, symptoms, breathing and swallowing function, genetic subtype, overall health, and treatment goals.
Can ALS be cured completely or stopped from progressing?
There is no cure for ALS, and treatments cannot completely stop disease progression. However, some treatments may help slow progression in selected patients, manage symptoms, support daily function, and improve quality of life.
Patients should work closely with a neurologist or ALS care team to review medications, supportive therapies, respiratory care, nutritional support, and suitable clinical trial options.
What is the best or newest treatment for ALS?
There is no single best treatment for every ALS patient. In Europe, riluzole is commonly used for eligible ALS patients, while tofersen, sold as Qalsody®, is available for adults with confirmed SOD1-associated ALS.
Tofersen was granted accelerated FDA approval on April 25, 2023, and received EU marketing authorization under exceptional circumstances in 2024. Edaravone is approved in some countries, including the United States, but is not currently authorized by the EMA as an ALS treatment in the EU.
What should someone do after an ALS diagnosis?
After an ALS diagnosis, patients should work with a neurologist or specialized ALS clinic to build a treatment and support plan. This may include medications, genetic testing, breathing monitoring, nutrition planning, mobility support, communication planning, symptom management, and clinical trial review.
Multidisciplinary care is often recommended because ALS affects movement, speech, swallowing, breathing, nutrition, emotional health, and daily independence. An ALS care team may include neurologists, rehabilitation specialists, speech-language pathologists, dietitians, respiratory therapists, social workers, palliative care specialists, and home care professionals.
When are feeding tubes or nutrition support considered in ALS?
Nutrition support may be considered when swallowing problems, weight loss, fatigue, or reduced appetite make it hard to maintain nutrition and hydration. A dietitian may recommend higher-calorie meals, texture-modified foods, thickened liquids, meal timing changes, or supplements when appropriate.
Feeding tubes may be discussed when swallowing becomes too difficult or unsafe. They can support hydration, nutrition, and medication intake while reducing some risks associated with difficult swallowing, such as choking or aspiration. The decision should be reviewed with the patient, family, neurologist, dietitian, and speech-language pathologist.
Will ALS patients need breathing support?
Some ALS patients require breathing support as the muscles involved in breathing weaken. This may include noninvasive ventilation, such as BiPAP, along with assisted coughing devices or suction devices to help clear secretions.
In advanced cases, mechanical ventilation through a tracheostomy may be considered. This is a major medical, lifestyle, and caregiver-support decision that should be reviewed early with the ALS care team.
Is stem cell therapy a treatment option for ALS?
Stem cell therapy for ALS remains experimental. It should not be described as a proven cure, a way to replace lost motor neurons, a way to stop ALS progression, or a replacement for standard neurological care.
Research is exploring whether stem cell-based and secretome-based approaches may influence neuroprotection, inflammatory signalling, cellular stress, paracrine signalling, and the biological environment around affected nerve cells. Suitability depends on individual medical review, and no responsible clinic should guarantee ALS improvement, disease stabilization, motor recovery, or survival extension from stem cell therapy.