REMCell Treatment for Spinal Cord Injury -
Robotics and Exosomes
Stem Cell Therapy for Spinal Cord Injury
The spinal cord is a column of nerve tissue that connects the brain with the peripheral nerves. Damage to the spinal cord can disrupt this communication, causing severe motor and sensory deficits that may lead to the inability to move or feel.
At ANOVA IRM in Offenbach, Germany, stem cell-based therapy is being explored as part of a regenerative treatment option for selected SCI patients. In collaboration with Cyberdyne Care Robotics, ANOVA offers REMCell, which combines stem cell-based neuro-regeneration with HAL exoskeleton training.
On this page, you will find more information about REMCell treatment and how stem cell therapy is being studied in relation to spinal cord injury. These options are still considered experimental. Outcomes vary from patient to patient, and treatment cannot guarantee restored movement, sensation, or functional recovery. An individual medical review is required to determine eligibility.
Spinal Cord Injury Treatment Overview
On this page, you can jump directly to the following topics:
- Stem cell therapy for spinal cord injury at ANOVA IRM
- Can stem cell therapy help spinal cord injury?
- ANOVA IRM treatment approach for spinal cord injury
- MSEC / Stem Cell Secretome therapy
- Bone Marrow Concentrate
- HAL exoskeleton rehabilitation
- REMCell combination treatment
- Candidate suitability and exclusion criteria
- Treatment workflow, timeline, travel, cost and insurance
- Precision diagnostics
- Targeted image-guided treatment
- How HAL neuro-functional training works
- Medical evaluation and FAQs
- References and further reading
Patients may be considered for treatment in selected cases involving:
- Partial or incomplete spinal cord injuries
- Cervical, thoracic, or lumbar spinal cord injuries
- Traumatic spinal injury
- Spinal cord compression
- Spinal cord edema after surgery
- Complete spinal cord injury only in selected responsive cases
Stem Cell Therapy for Spinal Cord Injury at ANOVA IRM
Stem cell therapy is not a replacement for established SCI treatment. Surgery, medication, physical therapy, and neuro-rehabilitation remain standard components of treating spinal cord injuries, but they often focus on stabilization and symptom management rather than biological repair.
Conventional neuro-rehabilitation has often been built on two assumptions:
- Further functional recovery was not possible during the chronic phase, starting one year after the SCI.
- The main problem in SCI patients occurs only at the spinal cord level.
Both assumptions have since been challenged, at least partially. By shifting focus beyond spinal stabilization alone, regenerative medicine at ANOVA IRM explores stem cell-based therapies in relation to inflammatory pathways and biological processes involved in the spinal cord injury environment.
This approach is combined with neuro-functional training through the HAL exoskeleton. Together, these two elements form REMCell, or Robotic Exoskeleton and Mesenchymal Stem Cell Therapy.
Since 2019, ANOVA IRM has offered this approach in collaboration with Cyberdyne Care Robotics, the developer of the HAL robotic exoskeleton.
Can Stem Cell Therapy Help Spinal Cord Injury?
Stem cell therapy for spinal cord injury is still considered experimental. It is not a cure for SCI, and outcomes vary from patient to patient. However, it is being explored because spinal cord injury often involves more than the initial mechanical damage.
In cases of trauma, compression, or fractured vertebrae, secondary damage may also occur in and around the spinal cord. This can involve:
- Inflammation, bleeding, edema, and swelling
- Increased pressure inside the spinal canal
- Reduced blood supply to damaged spinal cord tissue
- Disrupted axons, demyelination, and glial scarring
- Loss of neural and supporting cells
These processes can make spinal cord injury difficult to treat with local stabilization alone. Stem cell-based therapies are being studied because they may influence the damaged tissue environment through biological signalling, rather than simply replacing lost nerve cells.
Mesenchymal stem cells and their secretome may release bioactive molecules involved in inflammatory signalling and tissue-response pathways. This is one reason Stem Cell Secretome / Exosome therapy is especially relevant to SCI research.
At the same time, biological signalling may not translate into functional improvement by itself. This is why ANOVA IRM combines stem cell-based neuro-regeneration with neuro-functional rehabilitation through the HAL exoskeleton in selected patients.
ANOVA IRM Treatment Approach for Spinal Cord Injury
At ANOVA IRM, stem cell-based therapies for spinal cord injury are delivered in a regulated German medical setting. Products undergo quality control before treatment and are handled within ANOVA IRM’s controlled medical framework.
We employ only autologous treatment concepts, meaning therapies are based on the patient’s own biological material rather than donor-derived products.
Depending on the type of spinal cord injury, different stem cell types and stem cell-derived products may be considered. Treatment typically involves Mesenchymal Stem Cell Secretome (MSEC), Bone Marrow Concentrate (BMC), or a combination of the two.
What Therapeutic Outcomes Can Be Expected?
Stem cell-based therapy for spinal cord injury is still experimental, and results vary from patient to patient. At ANOVA IRM, the treatment concept is based on reviewing stem cell-based therapy together with neuro-functional rehabilitation.
External pre-clinical research on mesenchymal stem cells and their secretome has explored possible effects on damaged spinal cord tissue, including glial scar remodelling, vascularization, and axonal growth. These mechanisms are one reason MSEC / Secretome therapy is being explored for SCI.
During consultation, patients often ask about goals such as mobility with aids, greater independence, motor function, neuropathic pain, spasticity, sensitivity, and quality of life. These questions are reviewed individually based on the type and severity of injury, remaining nerve signals, overall health, and rehabilitation participation.
Pressure sore risk, sensitivity, mobility, and daily care needs can be discussed as part of the patient’s individual medical review.
While stem cell-based therapy and HAL exoskeleton training may be reviewed together as part of a rehabilitation-focused treatment plan, treatment remains experimental and cannot guarantee restored walking ability, symptom improvement, or full neurological recovery.
Potency Hypothesis of Stem Cell Therapies
Stem cells and their secretome may communicate with the damaged tissue environment, including immune cells. In spinal cord injury, this signalling is being studied in relation to inflammatory pathways and tissue-response processes around damaged tissue.
The goal of stem cell-based therapy is not simply to replace lost nerve cells. Instead, mesenchymal stem cells and their secretome are being explored for their potential to influence biological processes involved in the spinal cord injury environment.
For this reason, ANOVA IRM considers stem cell-based treatment and intensive rehabilitation together when reviewing selected SCI cases.
Mesenchymal Stem Cell Secretome / Exosome Therapy
Mesenchymal Stem Cell Secretome (MSEC) therapy is a cell-free stem cell-derived treatment. Instead of relying on living stem cells, this treatment uses the bioactive molecules released by mesenchymal stem cells, including exosomes, cytokines, proteins, growth factors, miRNA, and microvesicles.
At ANOVA IRM, MSEC is produced from the patient’s own adipose-derived stem cells, which are harvested from abdominal fat tissue through a limited liposuction procedure under light sedation.
Unlike localized BMC therapy, MSEC is administered intravenously as part of the treatment protocol. The final secretome product is separated from the living stem cells and passes through quality control before use.
A practical advantage of MSEC is that it can be stored after production. This allows ANOVA IRM to produce 10 injection doses from one liposuction and administer them over time.
This may be relevant for treatment planning in SCI cases where repeated applications are considered.

MSC Secretome / Exosome Therapy
Bone Marrow Concentrate
Autologous Bone Marrow Concentrate (BMC) may be used for locally restricted damage in SCI, especially when one vertebra or a defined treatment region is involved.
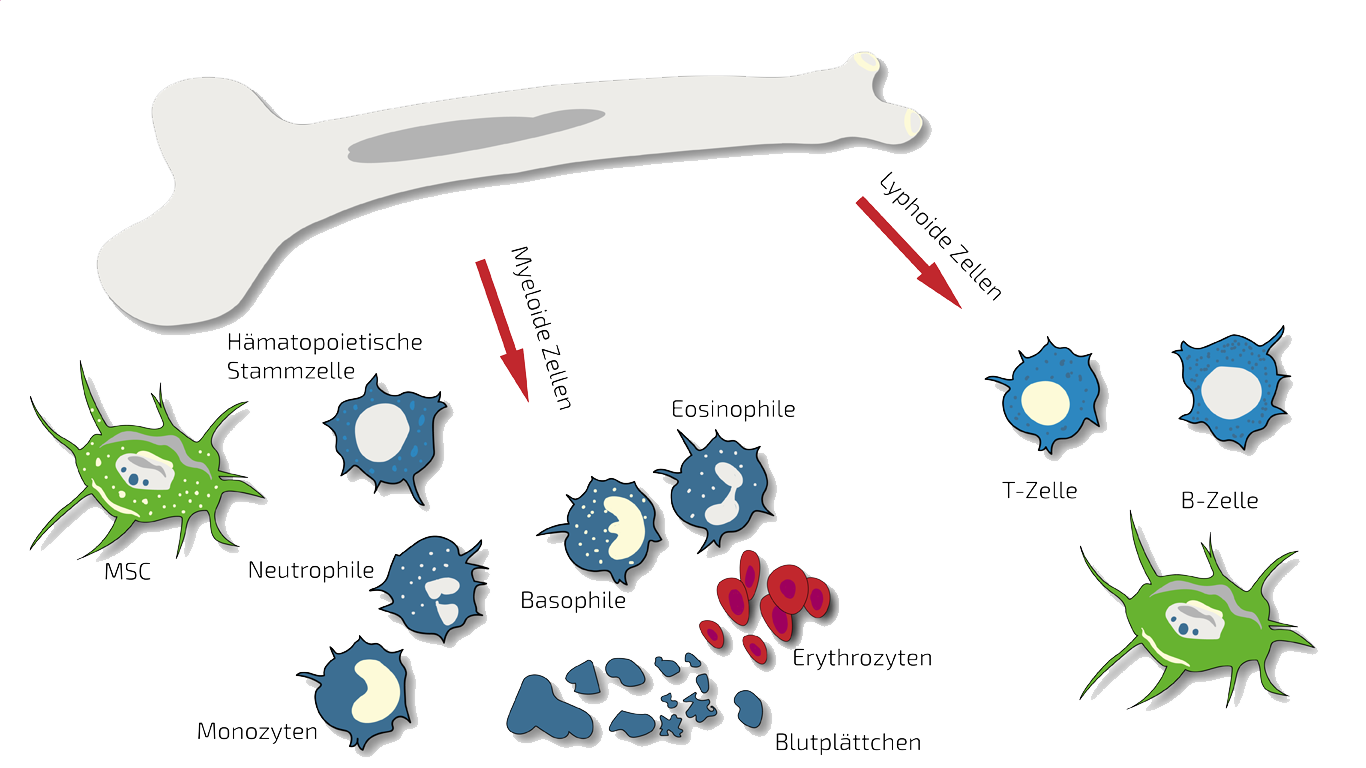
In these cases, ANOVA IRM can treat the affected region with targeted, localized BMC injections. BMC contains autologous adult stem cells, including hematopoietic and mesenchymal stem cells in their natural composition, which are isolated and concentrated from the patient’s pelvic crest in a short procedure under light sedation.
BMC may be considered in selected cases where the treatment plan focuses on a defined local spinal or vertebral target.
For ongoing therapy, BMC may be combined with MSEC treatment.
Bone Marrow Concentrate Therapy
HAL Exoskeleton Rehabilitation
Since 2019, ANOVA IRM has partnered with Cyberdyne Care Robotics to deliver functional training for spinal cord injury patients using the HAL® Hybrid Assistive Limb exoskeleton.
Cyberdyne’s state-of-the-art rehabilitation programs are used for intensive physiotherapy in incomplete or responsive SCI patients. To undergo HAL exoskeleton rehabilitation, patients must have measurable nerve signals during their first evaluation.
When these signals are present, HAL uses weak neurological impulses from the patient to help drive robotic movement and support neuro-functional feedback.
Training takes place at Cyberdyne’s German facility in Bochum. Patients typically train five days per week over the three-month program.

HAL Exoskeleton Training | © Cyberdyne
Combining Stem Cell Therapy With HAL Exoskeleton Training
At ANOVA IRM, stem cell-based therapies may be combined with Cyberdyne’s HAL Exoskeleton Rehabilitation through REMCell treatment.
This combination therapy is built on two principles:
- The potential immune-modulating and anti-inflammatory mechanisms being studied in stem cell-based therapy
- Neuro-functional training with the HAL exoskeleton using measurable residual neurological impulses
Stem cell therapy does not cure SCI. However, it may help improve the biological conditions needed for rehabilitation, especially when combined with intensive functional training.
HAL training takes place at Cyberdyne’s facility in Bochum. During the three-month REMCell program, patients return to Offenbach for continued stem cell-based treatment, with 10 MSEC doses typically administered every two weeks after production is complete.
REMCell should be understood as a possible pathway for selected patients, not as the standard treatment for every spinal cord injury case.
Contraindications
Our stem cell treatments are experimental, but we only treat patients for whom we believe the risk/benefit ratio indicates treatment based on the state of the art, i.e., medical, scientific evidence.
Please understand that we therefore do not treat patients for whom the following points apply:
- Active cancer in the last two years
- Not yet of legal age
- Existing pregnancy or lactation period
- Unable to breathe on own, ventilator
- Difficulty breathing in supine position
- Dysphagia (extreme difficulty swallowing)
- Psychiatric disorder
- Active infectious disease (Hepatitis A, B, C, HIV, Syphilis, or other)
Who May Be a Candidate for SCI Stem Cell Therapy?
As an experimental treatment, stem cell-based therapy is not suitable for every spinal cord injury patient. Suitability depends on the type of injury, remaining neurological function, overall health, and rehabilitation potential. An individual medical review is required to determine whether treatment may be appropriate.
Patients who may be considered include those with:
- Incomplete or partial spinal cord injuries
- Cervical, thoracic, or lumbar spinal cord injuries
- Spinal cord compression in selected cases
- Spinal cord edema after surgery in selected cases
- Chronic SCI with realistic expectations
- Complete SCI only in selected responsive cases
Treatment may not be suitable for patients with:
- No measurable residual nerve signaling, especially for REMCell/HAL treatment
- Active cancer within the last two years
- Active infectious disease
- Pregnancy or lactation
- Patients who are not legal adults
- Severe breathing difficulty or ventilator dependence
- Difficulty breathing while lying down
- Severe dysphagia
- Certain psychiatric disorders
- Expectations of a guaranteed cure or full reversal of paralysis
For REMCell and HAL exoskeleton training, weak residual neurological impulses must be present and measurable. For MSEC / Secretome therapy, the patient must also be medically suitable for autologous MSEC production.
Therapy Workflow for REMCell Treatment of Spinal Cord Injury
What to Expect From the Treatment Process
Step 1: Remote Medical Record Review
Before treatment planning can begin, ANOVA IRM must first determine candidacy. To make this as easy as possible, prospective patients can start a remote case review before travelling to Germany.
Patients can begin the process by submitting the contact form. Shortly after, they receive an email with condition-specific information, including the experimental nature of the treatment and possible next steps. Interested patients can request more information. A patient care manager will then reach out to arrange a video consultation.
In some cases, ANOVA IRM may ask patients to send relevant imaging. However, this is not required for the initial consultation.
Patient care managers can help explain what information is needed upfront and schedule a call with an ANOVA physician to determine whether the patient should proceed with in-person eligibility testing and treatment planning.
Patient care team support is free. Physician appointment charges may apply, but the consultation fee is credited toward treatment costs if the patient proceeds.
Step 2: Pre-Treatment Eligibility Testing
Once initial suitability appears possible, patients will be directed to complete pre-treatment eligibility testing.
This typically starts with preliminary bloodwork in the patient’s home country to check for exclusion criteria such as HIV, hepatitis, syphilis, or other active infectious diseases. Patients with certain medical or substance-related risk factors may also be excluded.
If these preliminary results do not show exclusion criteria, patients may then travel to ANOVA IRM in Offenbach, Germany. On the first day of treatment at ANOVA IRM, the required testing is repeated according to German medical and regulatory requirements to confirm that the patient’s cells can be used in the laboratory.
Step 3: REMCell Treatment Planning
ANOVA IRM prepares a treatment plan in collaboration with Cyberdyne Care Robotics. This can often be arranged before travel to Germany is required for stem cell harvesting.
ANOVA IRM follows established application schedules for stem cell-based treatment in SCI patients, so treatment can be coordinated with ongoing HAL training. While this combined approach is generally recommended when HAL training is part of the treatment plan, the schedule may be adjusted based on the patient’s medical needs, availability, and individual treatment plan.
Before treatment begins, the expected timeline and cost estimate are clarified with the patient.
Step 4: Stem Cell Harvesting and Production
Stem cell harvesting is conducted approximately four weeks before treatment. At this stage, patients come to ANOVA IRM for the required tissue collection.
For REMCell treatment, this usually involves a mini-liposuction procedure to collect adipose tissue from abdominal fat. The mesenchymal stem cells are then isolated, cultivated, and used to produce the stem cell secretome.
The final secretome product no longer contains living MSCs. It then undergoes quality control before being stored for treatment.
If BMC is included in the patient’s treatment plan, bone marrow may also be harvested from the pelvic crest.
Step 5: REMCell Workflow With HAL Exoskeleton Training
Stem cell therapy is planned to coincide with HAL exoskeleton training at Cyberdyne’s facility in Bochum. Training typically takes place five days per week during the three-month program.
Patients return to ANOVA IRM in Offenbach according to their treatment plan, typically every two weeks, to receive new secretome doses. In total, 10 MSEC doses are usually administered over the three-month program.
This means REMCell patients should expect regular travel between Bochum and Offenbach during the treatment period.
Treatment Timeline and Travel Requirements
Initial analysis and counselling can usually begin remotely, without travelling to Offenbach. This stage may take two weeks to several months, depending on patient availability and scheduling.
The main treatment timeline is usually built around three stages:
- Stem cell harvesting: Patients travel to ANOVA IRM in Offenbach for tissue collection. For MSEC / Secretome therapy, this usually involves approximately two consecutive days for adipose tissue harvesting and preparation.
- Secretome production: After harvesting, the stem cell secretome is produced and quality-controlled. This process takes approximately four weeks.
- REMCell treatment: REMCell includes a three-month HAL exoskeleton training program at Cyberdyne’s facility in Bochum. During this period, patients typically train five days per week and travel back to Offenbach for MSEC applications according to their treatment plan.
Because REMCell involves treatment in both Bochum and Offenbach, international patients should expect regular travel between the two locations during the treatment period. ANOVA IRM clarifies the expected timeline, number of visits, and travel requirements before treatment begins.
Cost of Stem Cell Therapy for Spinal Cord Injury
The cost of stem cell therapy for spinal cord injury depends on the patient’s condition, treatment plan, and whether HAL exoskeleton training is included.
When combined with HAL training, treatment may cost several tens of thousands of euros. Before treatment begins, ANOVA IRM provides an individual cost estimate so patients understand the expected cost of their treatment plan.
Does Health Insurance Cover the Therapy Costs?
Stem cell-based therapies for spinal cord injury are experimental and are generally not covered by health insurance.
Patients should expect to pay for treatment themselves unless their insurer confirms otherwise.
Why Choose ANOVA IRM for Spinal Cord Injury Treatment?
- Autologous therapies: Treatment uses the patient’s own biological material, including MSEC / Secretome therapy and BMC, where appropriate.
- REMCell combination treatment: Selected patients may combine stem cell-based therapy with HAL exoskeleton rehabilitation through Cyberdyne Care Robotics.
- Controlled treatment in Germany: Treatment takes place at ANOVA IRM in Offenbach am Main, with HAL training coordinated in Bochum.
- Individual medical review: Each patient is reviewed before treatment is recommended, with clear expectations around eligibility, timeline, cost, and experimental status.
How Does the ANOVA Therapy Differ? Precision Diagnostics for Individual Treatment Planning
Dr. mult. Michael K. Stehling, the founder of ANOVA IRM and the Vitus Prostate Center , is a radiologist (MD) and holds a PhD in physics. For this reason, the ANOVA Institute for Regenerative Medicine, in cooperation with the Prof. Stehling Institute for Diagnostic Imaging located in the same building, has the capability to use special precision diagnostics such as arthro-MRI and non-radioactive contrast MRIs.
Compared to many conventional MRIs, these methods are often able to localize the pain-causing inflammation, degeneration and damage in your spine and vertebrae. This enables us to determine individually how patients should be treated and where the stem cells should be applied.
Furthermore, in consultation with you and if necessary or advisable, we supplement our patient-specific diagnostics with specific blood tests on hormones, inflammation parameters and other factors that are important in your case, or recommend further examinations such as a preventive MRI spinal scan.

Precision MRI scans - find the source of pain
ANOVA IRM © Siemens Healthcare GmbH
How Does the ANOVA Therapy Differ? Targeted, Image-Guided Treatment
Based on our specific diagnostics using arthro-MRI and non-radioactive contrast medium MRIs, we can, in contrast to many other clinics, deliver the stem cells with image support, e.g. using CT, precisely to the affected area. This means we can inject into and at joints, vertebrae and ligaments to specifically and quickly trigger an effect where inflammation causes pain. All interventions are performed under supervision and care of our anesthesiologist and are pain free.
Of course, we will thoroughly advise you in the early process and the on-site consultation in advance on all steps and discuss alternatives and expectations.

CT-assisted stem cell injection into joints
ANOVA IRM © Siemens Healthcare GmbH
How HAL Neuro-Functional Training Works
This generates nerve signals in so-called proprioceptors in the muscles and joints, which are fed back to the brain (afferent signals). These afferent signals originating in the legs and going to the brain, and efferent signals, running down the spinal cord to the peripheral nerves form a feedback loop. In patients with SCI this feedback loop is interrupted and with time degenerates.
Functional MRI studies, which can visualize brain activity, have shown that the areas in the motor cortex of the brain (gyrus praecentralis), which control specific movements of the legs and are normally very focused on small areas of the motor cortex, "smear out" over larger areas in patients with SCI. This might impede voluntary initiation of motion by deeper functional centers of the brain.
During HAL training, the functional activity is refocused onto the original smaller areas. It thus appears that the re-establishment of the feedback loop, particularly the sensory input from the proprioceptors in the leg to the brain, is an essential component of voluntary motion.
Request a Medical Evaluation
Find out whether stem cell-based therapy may be suitable for your spinal cord injury.
ANOVA IRM can begin with a remote medical review before you travel to Germany. Our patient care team can explain the next steps and help arrange a physician consultation with Dr. Michael K. Stehling.
Because stem cell-based therapy for SCI is experimental, treatment can only be recommended after an individual medical review and benefit-risk assessment. ANOVA IRM cannot treat children or pregnant patients, and other medical factors may also exclude a patient from treatment.
Frequently Asked Questions About Stem Cell Therapy for Spinal Cord Injury
Is stem cell therapy for spinal cord injury available at ANOVA IRM?
Yes. ANOVA IRM offers stem cell-based therapy for selected spinal cord injury patients after medical review. Treatment may involve MSEC / Secretome therapy, Bone Marrow Concentrate, HAL exoskeleton rehabilitation, or a combination, depending on suitability.
Can stem cell therapy cure spinal cord injury?
No. Stem cell therapy is not an established cure for spinal cord injury, and treatment cannot guarantee restored walking ability, motor function, or full neurological recovery. At ANOVA IRM, stem cell-based therapy is considered experimental and can only be recommended after individual medical review.
Who is a candidate for SCI stem cell therapy?
Suitability depends on the type of injury, remaining neurological function, overall health, and rehabilitation potential. Patients with incomplete or partial spinal cord injuries may be more likely to be considered, while complete SCI is only considered in selected responsive cases.
What is MSEC / Stem Cell Secretome therapy?
MSEC stands for Mesenchymal Stem Cell Secretome. It is a cell-free therapy that uses the bioactive molecules released by mesenchymal stem cells, including exosomes and other signalling substances, rather than transplanting living stem cells directly.
What is REMCell therapy?
REMCell stands for Robotic Exoskeleton and Mesenchymal Stem Cell Therapy. It combines stem cell-based regenerative treatment at ANOVA IRM with HAL exoskeleton rehabilitation through Cyberdyne Care Robotics for selected patients with measurable residual nerve signals.
How long does treatment take?
The timeline depends on the treatment protocol. Initial review can begin remotely, while tissue harvesting and pre-treatment testing require travel to Offenbach. MSEC production takes approximately four weeks, and REMCell treatment with HAL training may involve a three-month program in Bochum with regular visits to Offenbach.
How much does stem cell therapy for spinal cord injury cost?
Costs depend on the patient’s condition, treatment plan, and whether HAL exoskeleton training is included. When combined with HAL training, treatment may cost several tens of thousands of euros. ANOVA IRM provides an individual cost estimate before treatment begins.
Does health insurance cover stem cell therapy for spinal cord injury?
Stem cell-based therapies for spinal cord injury are experimental and are generally not covered by health insurance. Patients should expect to pay for treatment themselves unless their insurer confirms otherwise.
Can international patients apply for treatment?
Yes. International patients can begin with a remote review before travelling to Germany. ANOVA IRM’s patient care team can explain what information is needed and help arrange the next steps for physician consultation, pre-treatment testing, and treatment planning.
Read More
Repair of injured spinal cord using biomaterial scaffolds and stem cells
Euro Stemcell foundation: How could stem cells help with spinal cord injuries
Paralysed man walks again after cell transplant
Christopher and Dana Reeve Foundation
Stem cell clinical trial aims to combat nerve damage in human tissue
Stem Cell Secretome for Spinal Cord Repair: Is It More than Just a Random Baseline Set of Factors?
References and Literature: Stem Cell-Based Therapies and Spinal Cord Injury
- Hejčl A, Sedy J, Kapcalova M, Toro DA, Amemori T, Lesny P, Likavcanova-Masinova K, Krumbholcova E, Pradny M, Michalek J, Burian M, Hajek M, Jendelova P, Sykova E. HPMA-RGD hydrogels seeded with mesenchymal stem cells improve functional outcome in chronic spinal cord injury. Stem Cells and Development. 2010;19:1535–1546.
- Anthony DF, Shiels PG. Exploiting paracrine mechanisms of tissue regeneration to repair damaged organs. Transplantation Research. 2013;2(1):10.
- Wright KT, Masri WE, Osman A, Chowdhury J, Johnson WEB. Concise review: Bone marrow for the treatment of spinal cord injury: mechanisms and clinical implications. Stem Cells. 2011;29:169–178.
- Quertainmont R, Cantinieaux D, Botman O, Eid S, Schoenen J, Franzen R. Mesenchymal stem cell graft improves recovery after spinal cord injury in adult rats through neurotrophic and pro-angiogenic actions. PLOS ONE. 2012;7.
- Lamichhane TN, et al. Emerging roles for extracellular vesicles in tissue engineering and regenerative medicine. Tissue Engineering Part B: Reviews. 2014;21(1):45–54.
- Thuret S, Moon LDF, Gage FH. Therapeutic interventions after spinal cord injury. Nature Reviews Neuroscience. 2006;7(8):628–643.
- Lindvall O, Kokaia Z. Stem cells for the treatment of neurological disorders. Nature. 2006;441(7097):1094–1096.
- Yoon SH, Shim YS, Park YH, Chung JK, Nam JH, Kim MO, Park HC, Park SR, Min BH, Kim EY, et al. Complete spinal cord injury treatment using autologous bone marrow cell transplantation and bone marrow stimulation with granulocyte macrophage-colony stimulating factor: Phase I/II clinical trial. Stem Cells. 2007;25(8):2066–2073.
- Karamouzian S, Nematollahi-Mahani SN, Nakhaee N, et al. Clinical safety and primary efficacy of bone marrow mesenchymal cell transplantation in subacute spinal cord injured patients. Clinical Neurology and Neurosurgery. 2012;114(7):935–939.
- Saito F, Nakatani T, Iwase M, et al. Spinal cord injury treatment with intrathecal autologous bone marrow stromal cell transplantation: the first clinical trial case report. Journal of Trauma. 2008;64(1):53–59.
- Saito F, Nakatani T, Iwase M, et al. Administration of cultured autologous bone marrow stromal cells into cerebrospinal fluid in spinal injury patients: a pilot study. Restorative Neurology and Neuroscience. 2012;30(2):127–136.
Further References About MSEC and Stem Cell Therapies for Spinal Cord Injuries
- Ramer LM, Ramer MS, Bradbury EJ. Restoring function after spinal cord injury: Towards clinical translation of experimental strategies. The Lancet Neurology. 2014;13:1241–1256. https://doi.org/10.1016/S1474-4422(14)70144-9
- Silva NA, Sousa N, Reis RL, Salgado AJ. From basics to clinical: A comprehensive review on spinal cord injury. Progress in Neurobiology. 2014;114:25–57. https://doi.org/10.1016/j.pneurobio.2013.11.002
- Bradbury EJ, Burnside ER. Moving beyond the glial scar for spinal cord repair. Nature Communications. 2019;10:3879. https://doi.org/10.1038/s41467-019-11707-7
- Schuld C, Franz S, Bruggemann K, Heutehaus L, Weidner N, Kirshblum SC, Rupp R, EMSCI Study Group. International standards for neurological classification of spinal cord injury: Impact of the revised worksheet (revision 02/13) on classification performance. Journal of Spinal Cord Medicine. 2016;39:504–512. https://doi.org/10.1080/10790268.2016.1180831
- Anderson DK, Means ED, Waters TR, Green ES. Microvascular perfusion and metabolism in injured spinal cord after methylprednisolone treatment. Journal of Neurosurgery. 1982;56:106–113. https://doi.org/10.3171/jns.1982.56.1.0106
- Oyinbo CA. Secondary injury mechanisms in traumatic spinal cord injury: A nugget of this multiply cascade. Acta Neurobiologiae Experimentalis. 2011;71:281–299.
- Kakulas BA. Neuropathology: The foundation for new treatments in spinal cord injury. Spinal Cord. 2004;42:549–563. https://doi.org/10.1038/sj.sc.3101670
- Rowland JW, Hawryluk GW, Kwon B, Fehlings MG. Current status of acute spinal cord injury pathophysiology and emerging therapies: Promise on the horizon. Neurosurgical Focus. 2008;25. https://doi.org/10.3171/FOC.2008.25.11.E2
- Donnelly DJ, Popovich PG. Inflammation and its role in neuroprotection, axonal regeneration and functional recovery after spinal cord injury. Experimental Neurology. 2008;209:378–388. https://doi.org/10.1016/j.expneurol.2007.06.009
- Pires AO, Mendes-Pinheiro B, Teixeira FG, Anjo SI, Ribeiro-Samy S, Gomes ED, Serra SC, Silva NA, Manadas B, Sousa N, et al. Unveiling the differences of secretome of human bone marrow mesenchymal stem cells, adipose tissue-derived stem cells, and human umbilical cord perivascular cells: A proteomic analysis. Stem Cells and Development. 2016;25:1073–1083. https://doi.org/10.1089/scd.2016.0048
- Nagoshi N, Nakashima H, Fehlings MG. Riluzole as a neuroprotective drug for spinal cord injury: From bench to bedside. Molecules. 2015;20:7775–7789. https://doi.org/10.3390/molecules20057775
- Salewski RP, Mitchell RA, Li L, Shen C, Milekovskaia M, Nagy A, Fehlings MG. Transplantation of induced pluripotent stem cell-derived neural stem cells mediate functional recovery following thoracic spinal cord injury through remyelination of axons. Stem Cells Translational Medicine. 2015;4:743–754. https://doi.org/10.5966/sctm.2014-0236
- Zakrzewski W, Dobrzynski M, Szymonowicz M, Rybak Z. Stem cells: Past, present, and future. Stem Cell Research & Therapy. 2019;10:68. https://doi.org/10.1186/s13287-019-1165-5
- Chen CJ, Ou YC, Liao SL, Chen WY, Chen SY, Wu CW, Wang CC, Wang WY, Huang YS, Hsu SH. Transplantation of bone marrow stromal cells for peripheral nerve repair. Experimental Neurology. 2007;204:443–453. https://doi.org/10.1016/j.expneurol.2006.12.004
Literature on HAL Training and Spinal Cord Injury Rehabilitation
- Grasmücke D, Zieriacks A, Jansen O, Fisahn C, Sczesny-Kaiser M, Wessling M, Meindl RC, Schildhauer TA, Aach M. Against the odds: what to expect in rehabilitation of chronic spinal cord injury with a neurologically controlled Hybrid Assistive Limb exoskeleton. A subgroup analysis of 55 patients according to age and lesion level. Neurosurgical Focus. 2017;42(5). https://doi.org/10.3171/2017.2.FOCUS171
- Brinkemper A, Grasmücke D, Yilmaz E, Reinecke F, Schildhauer TA, Aach M. Influence of locomotion therapy with the wearable cyborg HAL on bladder and bowel function in acute and chronic SCI patients. Global Spine Journal. 2021. https://doi.org/10.1177/21925682211003851
- Jansen O, Schildhauer TA, Meindl RC, Tegenthoff M, Schwenkreis T, Sczesny-Kaiser M, Grasmücke D, Fisahn C, Aach M. Functional outcome of neurologic-controlled HAL-exoskeletal neurorehabilitation in chronic spinal cord injury: A pilot with one year treatment and variable treatment frequency. Global Spine Journal. 2017. https://doi.org/10.1177/2192568217713754
- Jansen O, Grasmücke D, Meindl RC, Tegenthoff M, Schwenkreis P, Sczesny-Kaiser M, Wessling M, Schildhauer TA, Fisahn C, Aach M. Hybrid Assistive Limb exoskeleton HAL in the rehabilitation of chronic spinal cord injury: Proof of concept; the results in 21 patients. World Neurosurgery. 2018. https://doi.org/10.1016/j.wneu.2017.10.080
- Sczesny-Kaiser M, Höffken O, Aach M, Cruciger O, Grasmücke D, Meindl R, Schildhauer TA, Schwenkreis P, Tegenthoff M. HAL® exoskeleton training improves walking parameters and normalizes cortical excitability in primary somatosensory cortex in spinal cord injury patients. Journal of NeuroEngineering and Rehabilitation. 2015. https://doi.org/10.1186/s12984-015-0058-9
- Aach M, Cruciger O, Sczesny-Kaiser M, Höffken O, Meindl RC, Tegenthoff M, Schwenkreis P, Sankai Y, Schildhauer TA. Voluntary driven exoskeleton as a new tool for rehabilitation in chronic spinal cord injury: A pilot study. The Spine Journal. 2014. https://doi.org/10.1016/j.spinee.2014.03.042
- Puentes S, Kadone H, Kubota S, Abe T, Shimizu Y, Marushima A, Sankai Y, Yamazaki M, Suzuki K. Reshaping of gait coordination by robotic intervention in myelopathy patients after surgery. Frontiers in Neuroscience. 2018. https://doi.org/10.3389/fnins.2018.00099
- Cruciger O, Schildhauer TA, Meindl RC, Tegenthoff M, Schwenkreis P, Citak M, Aach M. Impact of locomotion training with a neurologic controlled hybrid assistive limb (HAL) exoskeleton on neuropathic pain and health-related quality of life (HRQoL) in chronic SCI: A case study. Disability and Rehabilitation: Assistive Technology. 2014. https://doi.org/10.3109/17483107.2014.981875
Further References for MSC, BMC, Stemcell Secretome and EVs
- Georg Hansmann, Philippe Chouvarine, Franziska Diekmann, Martin Giera, Markus Ralser, Michael Mülleder, Constantin von Kaisenberg, Harald Bertram, Ekaterina Legchenko & Ralf Hass "Human umbilical cord mesenchymal stem cell-derived treatment of severe pulmonary arterial hypertension". Nature Cardiovascular Research volume 1, pages568–576 (2022).
- Murphy JM, Fink DJ, Hunziker EB, et al. Stem cell therapy in a caprine model of osteoarthritis . Arthritis Rheum. 2003;48:3464–74.
- Lee KB, Hui JH, Song IC, Ardany L, et al. Injectable mesenchymal stem cell therapy for large cartilage defects—a porcine model. Stem Cell. 2007;25:2964–71.
- Saw KY, Hussin P, Loke SC, et al. Articular cartilage regeneration with autologous marrow aspirate and hyaluronic acid: an experimental study in a goat model. Arthroscopy . 2009;25(12):1391–400.
- Black L, Gaynor J, Adams C, et al. Effect of intra-articular injection of autologous adipose-derived mesenchymal stem and regenerative cells on clinical signs of chronic osteoarthritis of the elbow joint in dogs. Vet Ther. 2008;9:192-200.
- Centeno C, Busse D, Kisiday J, et al. Increased knee cartilage volume in degenerative joint disease using percutaneously implanted, autologous mesenchymal stem cells. Pain Physician. 2008;11(3):343–53.
- Centeno C, Kisiday J, Freeman M, et al. Partial regeneration of the human hip via autologous bone marrow nucleated cell transfer: a case study. Pain Physician. 2006;9:253–6.
- Centeno C, Schultz J, Cheever M. Safety and complications reporting on the re-implantation of culture-expanded mesenchymal stem cells using autologous platelet lysate technique. Curr Stem Cell. 2011;5(1):81–93.
- Pak J. Regeneration of human bones in hip osteonecrosis and human cartilage in knee osteoarthritis with autologous adipose derived stem cells: a case series. J Med Case Rep. 2001;5:296.
- Kuroda R, Ishida K, et al. Treatment of a full-thickness articular cartilage defect in the femoral condyle of an athlete with autologous bone-marrow stromal cells. Osteoarthritis Cartilage. 2007;15:226–31.
- Emadedin M, Aghdami N, Taghiyar L, et al. Intra-articular injection of autologous mesenchymal stem cells in six patients with knee osteoarthritis. Arch Iran Med. 2012;15(7):422–8.
- Saw KY et al. Articular cartilage regeneration with autologous peripheral blood stem cells versus hyaluronic acid: a randomized controlled trial. Arthroscopy. 2013;29(4):684–94.
- Vangsness CT, Farr J, Boyd J, et al. Adult human mesenchymal stem cells delivered via intra-articular injection to the knee following partial medial meniscectomy. J Bone Joint Surg. 2014;96(2):90–8.
- Freitag, Julien, et al. Mesenchymal stem cell therapy in the treatment of osteoarthritis: reparative pathways, safety and efficacy–a review. BMC musculoskeletal disorders 17.1 (2016): 230.
- Maumus, Marie, Christian Jorgensen, and Danièle Noël. " Mesenchymal stem cells in regenerative medicine applied to rheumatic diseases: role of secretome and exosomes. " Biochimie 95.12 (2013): 2229-2234.
- Dostert, Gabriel, et al. " How do mesenchymal stem cells influence or are influenced by microenvironment through extracellular vesicles communication?. " Frontiers in Cell and Developmental Biology 5 (2017).
- Chaparro, Orlando, and Itali Linero. " Regenerative Medicine: A New Paradigm in Bone Regeneration. " (2016).
- Toh, Wei Seong, et al. " MSC exosome as a cell-free MSC therapy for cartilage regeneration: Implications for osteoarthritis treatment. " Seminars in Cell & Developmental Biology. Academic Press, 2016.
- Chaparro, Orlando, and Itali Linero. " Regenerative Medicine: A New Paradigm in Bone Regeneration. " (2016).
- S. Koelling, J. Kruegel, M. Irmer, J.R. Path, B. Sadowski, X. Miro, et al., Migratory chondrogenic progenitor cells from repair tissue during the later stages of human osteoarthritis , Cell Stem Cell 4 (2009) 324–335.
- B.A. Jones, M. Pei, Synovium-Derived stem cells: a tissue-Specific stem cell for cartilage engineering and regeneration , Tissue Eng. B: Rev. 18 (2012) 301–311.
- W. Ando, J.J. Kutcher, R. Krawetz, A. Sen, N. Nakamura, C.B. Frank, et al., Clonal analysis of synovial fluid stem cells to characterize and identify stable mesenchymal stromal cell/mesenchymal progenitor cell phenotypes in a porcine model: a cell source with enhanced commitment to the chondrogenic lineage, Cytotherapy 16 (2014) 776–788.
- K.B.L. Lee, J.H.P. Hui, I.C. Song, L. Ardany, E.H. Lee, Injectable mesenchymal stem cell therapy for large cartilage defects—a porcine model, Stem Cells 25 (2007) 2964–2971.
- W.-L. Fu, C.-Y. Zhou, J.-K. Yu, A new source of mesenchymal stem cells for articular cartilage repair: mSCs derived from mobilized peripheral blood share similar biological characteristics in vitro and chondrogenesis in vivo as MSCs from bone marrow in a rabbit model , Am. J. Sports Med. 42 (2014) 592–601.
- X. Xie, Y. Wang, C. Zhao, S. Guo, S. Liu, W. Jia, et al., Comparative evaluation of MSCs from bone marrow and adipose tissue seeded in PRP-derived scaffold for cartilage regeneration , Biomaterials 33 (2012) 7008–7018.
- E.-R. Chiang, H.-L. Ma, J.-P. Wang, C.-L. Liu, T.-H. Chen, S.-C. Hung, Allogeneic mesenchymal stem cells in combination with hyaluronic acid for the treatment of osteoarthritis in rabbits , PLoS One 11 (2016) e0149835.
- H. Nejadnik, J.H. Hui, E.P. Feng Choong, B.-C. Tai, E.H. Lee, Autologous bone marrow–derived mesenchymal stem cells versus autologous chondrocyte implantation: an observational cohort study , Am. J. Sports Med. 38 (2010) 1110–1116.
- I. Sekiya, T. Muneta, M. Horie, H. Koga, Arthroscopic transplantation of synovial stem cells improves clinical outcomes in knees with cartilage defects , Clin. Orthop. Rel. Res. 473 (2015) 2316–2326.
- Y.S. Kim, Y.J. Choi, Y.G. Koh, Mesenchymal stem cell implantation in knee osteoarthritis: an assessment of the factors influencing clinical outcomes , Am. J. Sports Med. 43 (2015) 2293–2301.
- W.-L. Fu, Y.-F. Ao, X.-Y. Ke, Z.-Z. Zheng, X. Gong, D. Jiang, et al., Repair of large full-thickness cartilage defect by activating endogenous peripheral blood stem cells and autologous periosteum flap transplantation combined with patellofemoral realignment , Knee 21 (2014) 609–612.
- Y.-G. Koh, O.-R. Kwon, Y.-S. Kim, Y.-J. Choi, D.-H. Tak, Adipose-derived mesenchymal stem cells with microfracture versus microfracture alone: 2-year follow-up of a prospective randomized trial , Arthrosc. J. Arthrosc. Relat. Surg. 32 (2016) 97–109.
- T.S. de Windt, L.A. Vonk, I.C.M. Slaper-Cortenbach, M.P.H. van den Broek, R. Nizak, M.H.P. van Rijen, et al., Allogeneic mesenchymal stem cells stimulate cartilage regeneration and are safe for single-Stage cartilage repair in humans upon mixture with recycled autologous chondrons , Stem Cells (2016) (n/a-n/a).
- L. da Silva Meirelles, A.M. Fontes, D.T. Covas, A.I. Caplan, Mechanisms involved in the therapeutic properties of mesenchymal stem cells , Cytokine Growth Factor Rev. 20 (2009) 419–427.
- W.S. Toh, C.B. Foldager, M. Pei, J.H.P. Hui, Advances in mesenchymal stem cell-based strategies for cartilage repair and regeneration , Stem Cell Rev. Rep. 10 (2014) 686–696.
- R.C. Lai, F. Arslan, M.M. Lee, N.S.K. Sze, A. Choo, T.S. Chen, et al., Exosome secreted by MSC reduces myocardial ischemia/reperfusion injury , Stem Cell Res. 4 (2010) 214–222.
- S. Zhang, W.C. Chu, R.C. Lai, S.K. Lim, J.H.P. Hui, W.S. Toh, Exosomes derived from human embryonic mesenchymal stem cells promote osteochondral regeneration, Osteoarthr . Cartil. 24 (2016) 2135–2140.
- S. Zhang, W. Chu, R. Lai, J. Hui, E. Lee, S. Lim, et al., 21 – human mesenchymal stem cell-derived exosomes promote orderly cartilage regeneration in an immunocompetent rat osteochondral defect model , Cytotherapy 18 (2016) S13.
- C.T. Lim, X. Ren, M.H. Afizah, S. Tarigan-Panjaitan, Z. Yang, Y. Wu, et al., Repair of osteochondral defects with rehydrated freeze-dried oligo[poly(ethylene glycol) fumarate] hydrogels seeded with bone marrow mesenchymal stem cells in a porcine model
- A. Gobbi, G. Karnatzikos, S.R. Sankineani, One-step surgery with multipotent stem cells for the treatment of large full-thickness chondral defects of the knee , Am. J. Sports Med. 42 (2014) 648–657.
- A. Gobbi, C. Scotti, G. Karnatzikos, A. Mudhigere, M. Castro, G.M. Peretti, One-step surgery with multipotent stem cells and Hyaluronan-based scaffold for the treatment of full-thickness chondral defects of the knee in patients older than 45 years , Knee Surg. Sports Traumatol. Arthrosc. (2016) 1–8.
- A. Gobbi, G. Karnatzikos, C. Scotti, V. Mahajan, L. Mazzucco, B. Grigolo, One-step cartilage repair with bone marrow aspirate concentrated cells and collagen matrix in full-thickness knee cartilage lesions: results at 2-Year follow-up , Cartilage 2 (2011) 286–299.
- K.L. Wong, K.B.L. Lee, B.C. Tai, P. Law, E.H. Lee, J.H.P. Hui, Injectable cultured bone marrow-derived mesenchymal stem cells in varus knees with cartilage defects undergoing high tibial osteotomy: a prospective, randomized controlled clinical trial with 2 years’ follow-up , Arthrosc. J. Arthrosc. Relat. Surg. 29 (2013) 2020–2028.
- J.M. Hare, J.E. Fishman, G. Gerstenblith, et al., Comparison of allogeneic vs autologous bone marrow–derived mesenchymal stem cells delivered by transendocardial injection in patients with ischemic cardiomyopathy: the poseidon randomized trial, JAMA 308 (2012) 2369–2379.
- L. Wu, J.C.H. Leijten, N. Georgi, J.N. Post, C.A. van Blitterswijk, M. Karperien, Trophic effects of mesenchymal stem cells increase chondrocyte proliferation and matrix formation , Tissue Eng. A 17 (2011) 1425–1436.
- L. Wu, H.-J. Prins, M.N. Helder, C.A. van Blitterswijk, M. Karperien, Trophic effects of mesenchymal stem cells in chondrocyte Co-Cultures are independent of culture conditions and cell sources , Tissue Eng. A 18 (2012) 1542–1551.
- S.K. Sze, D.P.V. de Kleijn, R.C. Lai, E. Khia Way Tan, H. Zhao, K.S. Yeo, et al., Elucidating the secretion proteome of human embryonic stem cell-derived mesenchymal stem cells , Mol. Cell. Proteomics 6 (2007) 1680–1689.
- M.B. Murphy, K. Moncivais, A.I. Caplan, Mesenchymal stem cells: environmentally responsive therapeutics for regenerative medicine , Exp. Mol. Med. 45 (2013) e54.
- M.J. Lee, J. Kim, M.Y. Kim, Y.-S. Bae, S.H. Ryu, T.G. Lee, et al., Proteomic analysis of tumor necrosis factor--induced secretome of human adipose tissue-derived mesenchymal stem cells , J. Proteome Res. 9 (2010) 1754–1762.
- S. Bruno, C. Grange, M.C. Deregibus, R.A. Calogero, S. Saviozzi, F. Collino, et al., Mesenchymal stem cell-derived microvesicles protect against acute tubular injury, J. Am. Soc. Nephrol. 20 (2009) 1053–1067.
- M. Yá˜nez-Mó, P.R.-M. Siljander, Z. Andreu, A.B. Zavec, F.E. Borràs, E.I. Buzas, et al. Biological properties of extracellular vesicles and their physiological functions (2015).
- C. Lawson, J.M. Vicencio, D.M. Yellon, S.M. Davidson, Microvesicles and exosomes: new players in metabolic and cardiovascular disease , J. Endocrinol. 228 (2016) R57–R71.
- A.G. Thompson, E. Gray, S.M. Heman-Ackah, I. Mager, K. Talbot, S.E. Andaloussi, et al., Extracellular vesicles in neurodegenerative diseas—pathogenesis to biomarkers, Nat. Rev. Neurol. 12 (2016) 346–357.
- I.E.M. Bank, L. Timmers, C.M. Gijsberts, Y.-N. Zhang, A. Mosterd, J.-W. Wang, et al., The diagnostic and prognostic potential of plasma extracellular vesicles for cardiovascular disease , Expert Rev. Mol. Diagn. 15 (2015) 1577–1588.
- T. Kato, S. Miyaki, H. Ishitobi, Y. Nakamura, T. Nakasa, M.K. Lotz, et al., Exosomes from IL-1 stimulated synovial fibroblasts induce osteoarthritic changes in articular chondrocytes , Arthritis. Res. Ther. 16 (2014) 1–11.
- R.W.Y. Yeo, S.K. Lim, Exosomes and their therapeutic applications, in: C. Gunther, A. Hauser, R. Huss (Eds.), Advances in Pharmaceutical Cell TherapyPrinciples of Cell-Based Biopharmaceuticals, World Scientific, Singapore, 2015, pp. 477–491.
- X. Qi, J. Zhang, H. Yuan, Z. Xu, Q. Li, X. Niu, et al., Exosomes secreted by human-Induced pluripotent stem cell-derived mesenchymal stem cells repair critical-sized bone defects through enhanced angiogenesis and osteogenesis in osteoporotic rats , Int. J. Biol. Sci. 12 (2016) 836–849.
- R.C. Lai, F. Arslan, S.S. Tan, B. Tan, A. Choo, M.M. Lee, et al., Derivation and characterization of human fetal MSCs: an alternative cell source for large-scale production of cardioprotective microparticles , J. Mol. Cell. Cardiol. 48 (2010) 1215–1224.
- Y. Zhou, H. Xu, W. Xu, B. Wang, H. Wu, Y. Tao, et al., Exosomes released by human umbilical cord mesenchymal stem cells protect against cisplatin-induced renal oxidative stress and apoptosis in vivo and in vitro , Stem Cell Res. Ther. 4 (2013) 1–13.
- Y. Qin, L. Wang, Z. Gao, G. Chen, C. Zhang, Bone marrow stromal/stem cell-derived extracellular vesicles regulate osteoblast activity and differentiation in vitro and promote bone regeneration in vivo , Sci. Rep. 6 (2016) 21961.
- M. Nakano, K. Nagaishi, N. Konari, Y. Saito, T. Chikenji, Y. Mizue, et al., Bone marrow-derived mesenchymal stem cells improve diabetes-induced cognitive impairment by exosome transfer into damaged neurons and astrocytes , Sci. Rep. 6 (2016) 24805.
- K. Nagaishi, Y. Mizue, T. Chikenji, M. Otani, M. Nakano, N. Konari, et al., Mesenchymal stem cell therapy ameliorates diabetic nephropathy via the paracrine effect of renal trophic factors including exosomes , Sci. Rep. 6 (2016) 34842.
- S.R. Baglio, K. Rooijers, D. Koppers-Lalic, F.J. Verweij, M. Pérez Lanzón, N. Zini, et al., Human bone marrow- and adipose-mesenchymal stem cells secrete exosomes enriched in distinctive miRNA and tRNA species , Stem Cell Res. Ther. 6 (2015) 1–20.
- T. Chen, R. Yeo, F. Arslan, Y. Yin, S. Tan, Efficiency of exosome production correlates inversely with the developmental maturity of MSC donor, J. Stem Cell Res. Ther. 3 (2013) 2.
- R.C. Lai, S.S. Tan, B.J. Teh, S.K. Sze, F. Arslan, D.P. de Kleijn, et al., Proteolytic potential of the MSC exosome proteome: implications for an exosome-mediated delivery of therapeutic proteasome , Int. J. Proteomics 2012 (2012) 971907.
- T.S. Chen, R.C. Lai, M.M. Lee, A.B.H. Choo, C.N. Lee, S.K. Lim, Mesenchymal stem cell secretes microparticles enriched in pre-microRNAs , Nucleic Acids Res. 38 (2010) 215–224.
- R.W. Yeo, R.C. Lai, K.H. Tan, S.K. Lim, Exosome: a novel and safer therapeutic refinement of mesenchymal stem cell, J. Circ. Biomark. 1 (2013) 7.
- R.C. Lai, R.W. Yeo, S.K. Lim, Mesenchymal stem cell exosomes, Semin. Cell Dev. Biol. 40 (2015) 82–88.
- B. Zhang, R.W. Yeo, K.H. Tan, S.K. Lim, Focus on extracellular vesicles: therapeutic potential of stem cell-derived extracellular vesicles , Int. J. Mol. Sci. 17 (2016) 174.
- Hu G-w, Q. Li, X. Niu, B. Hu, J. Liu, Zhou S-m, et al., Exosomes secreted by human-induced pluripotent stem cell-derived mesenchymal stem cells attenuate limb ischemia by promoting angiogenesis in mice , Stem Cell Res. Ther. 6 (2015) 1–15.
- J. Zhang, J. Guan, X. Niu, G. Hu, S. Guo, Q. Li, et al., Exosomes released from human induced pluripotent stem cells-derived MSCs facilitate cutaneous wound healing by promoting collagen synthesis and angiogenesis , J. Transl. Med. 13 (2015) 1–14.
- B. Zhang, M. Wang, A. Gong, X. Zhang, X. Wu, Y. Zhu, et al., HucMSC-exosome mediated-Wnt4 signaling is required for cutaneous wound healing, Stem Cells 33 (2015) 2158–2168.
- B. Zhang, Y. Yin, R.C. Lai, S.S. Tan, A.B.H. Choo, S.K. Lim, Mesenchymal stem cells secrete immunologically active exosomes , Stem Cells Dev. 23 (2013) 1233–1244.
- C.Y. Tan, R.C. Lai, W. Wong, Y.Y. Dan, S.-K. Lim, H.K. Ho, Mesenchymal stem cell-derived exosomes promote hepatic regeneration in drug-induced liver injury models , Stem Cell Res. Ther. 5 (2014) 1–14.
- C. Lee, S.A. Mitsialis, M. Aslam, S.H. Vitali, E. Vergadi, G. Konstantinou, et al., Exosomes mediate the cytoprotective action of mesenchymal stromal cells on hypoxia-induced pulmonary hypertension , Circulation 126 (2012) 2601–2611.
- B. Yu, H. Shao, C. Su, Y. Jiang, X. Chen, L. Bai, et al., Exosomes derived from MSCs ameliorate retinal laser injury partially by inhibition of MCP-1 , Sci. Rep. 6 (2016) 34562.
- Jo CH, Lee YG, Shin WH, et al. Intra-articular injection of mesenchymal stem cells for the treatment of osteoarthritis of the knee: a proof of concept clinical trial. Stem Cells. 2014;32(5):1254–66.
- Vega, Aurelio, et al. Treatment of knee osteoarthritis with allogeneic bone marrow mesenchymal stem cells: a randomized controlled trial. Transplantation. 2015;99(8):1681–90.
- Davatchi F, Sadeghi-Abdollahi B, Mohyeddin M, et al. Mesenchymal stem cell therapy for knee osteoarthritis. Preliminary report of four patients. Int J Rheum Dis. 2011;14(2):211–5
- Hernigou P, Flouzat Lachaniette CH, Delambre J, et al. Biologic augmentation of rotator cuff repair with mesenchymal stem cells during arthroscopy improves healing and prevents further tears: a case- controlled study. Int Orthop. 2014;38(9):1811–1818
- Galli D, Vitale M, Vaccarezza M. Bone marrow-derived mesenchymal cell differentiation toward myogenic lineages: facts and perspectives. Biomed Res Int. 2014;2014:6.
- Beitzel K, Solovyova O, Cote MP, et al. The future role of mesenchymal Stem cells in The management of shoulder disorders . Arthroscopy. 2013;29(10):1702–1711.
- Isaac C, Gharaibeh B, Witt M, Wright VJ, Huard J. Biologic approaches to enhance rotator cuff healing after injury. J Shoulder Elbow Surg. 2012;21(2):181–190.
- Malda, Jos, et al. " Extracellular vesicles [mdash] new tool for joint repair and regeneration. " Nature Reviews Rheumatology (2016).
Further References about PRP
- Rubio-Azpeitia E, Andia I. Partnership between platelet-rich plasma and mesenchymal stem cells: in vitro experience. Muscles Ligaments Tendons J. 2014;4(1):52–62.
Extras
- Xu, Ming, et al. " Transplanted senescent cells induce an osteoarthritis-like condition in mice. " The Journals of Gerontology Series A: Biological Sciences and Medical Sciences (2016): glw154.
- McCulloch, Kendal, Gary J. Litherland, and Taranjit Singh Rai. " Cellular senescence in osteoarthritis pathology ." Aging Cell (2017).
Contraindications
Our stem cell treatments are experimental, but we only treat patients for whom we believe the risk/benefit ratio indicates treatment based on the state of the art, i.e., medical, scientific evidence.
Please understand that we therefore do not treat patients for whom the following points apply:
- Active cancer in the last two years
- Not yet of legal age
- Existing pregnancy or lactation period
- Unable to breathe on own, ventilator
- Difficulty breathing in supine position
- Dysphagia (extreme difficulty swallowing)
- Psychiatric disorder
- Active infectious disease (Hepatitis A, B, C, HIV, Syphilis, or other)